Panchabhai Tanmay S, Patil Pradnya D, Riley Elizabeth C, Mitchell Charlene K
Norton Thoracic Institute, St. Joseph's Hospital and Medical Center, Phoenix, AZ, USA.
Department of Hospital Medicine, Medicine Institute, Cleveland Clinic, Cleveland, OH, USA.
Int J Crit Illn Inj Sci. 2016 Apr-Jun;6(2):89-92. doi: 10.4103/2229-5151.183026.
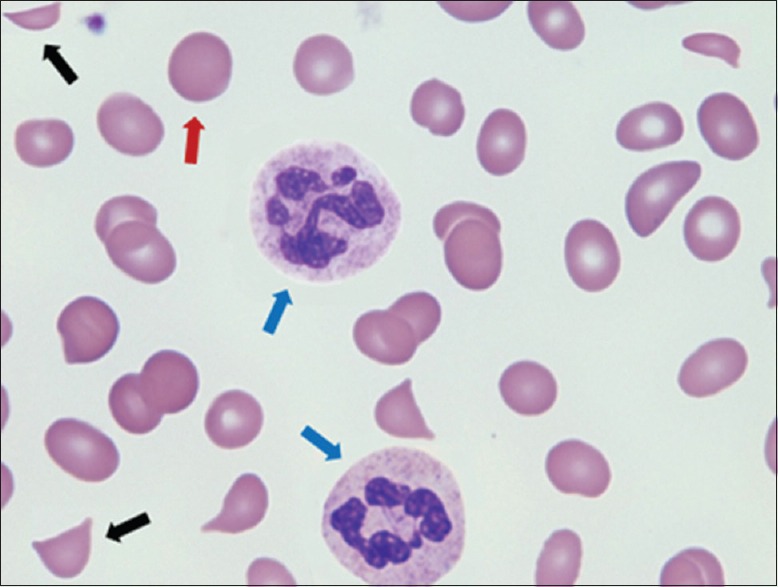
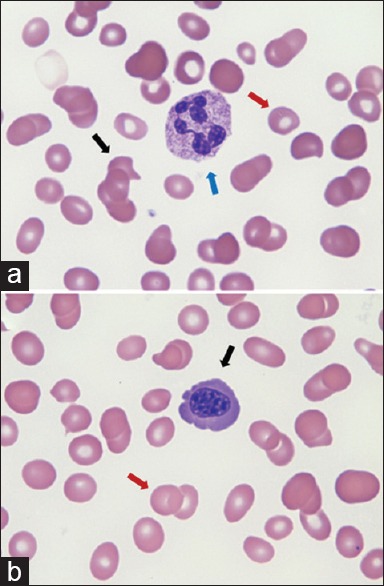
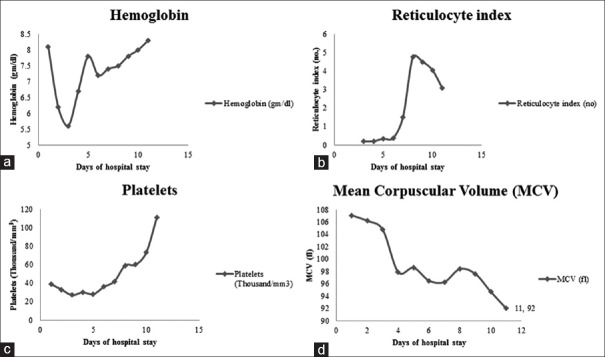
Thrombotic thrombocytopenic purpura (TTP) has high mortality and necessitates prompt recognition of microangiopathic hemolytic anemia (MAHA) and initiation of plasmapheresis. We present a challenging diagnostic workup and management of a 42-year-old man who presented with anemia, thrombocytopenia, and schistocytes on peripheral smear, all pointing to MAHA. Plasmapheresis and steroid therapy were promptly initiated, but hemolysis continued. Further workup showed megaloblastic anemia, severe Vitamin B12 deficiency, high iron saturation, and absent reticulocytosis, none of which could be explained by TTP. Severe Vitamin B12 deficiency can lead to hemolytic anemia from the destruction of red cells in the marrow that have failed the process of maturation. However, this should not cause thrombotic microangiopathy. Previous reports of B12 deficiency presenting with MAHA and a TTP-like manifestation have identified acute hyperhomocysteinemia as a missing link between B12 deficiency and MAHA, so this possibility was further explored. Our patient similarly had significantly elevated serum homocysteine levels, confirming this suspicion of Vitamin B12 deficiency. Vitamin B12 replacement led to normalization of the elevated levels of homocysteine, the disappearance of schistocytes on the peripheral smear, and resolution of the microangiopathic hemolysis, thereby confirming the diagnosis. It is pertinent that intensivists not only know the importance of early recognition and treatment of TTP but are also familiar with rare conditions that can present in a similar fashion.
血栓性血小板减少性紫癜(TTP)死亡率高,需要及时识别微血管病性溶血性贫血(MAHA)并启动血浆置换。我们介绍了一名42岁男性具有挑战性的诊断检查和治疗过程,该患者表现为贫血、血小板减少以及外周血涂片出现裂体细胞,所有这些都指向MAHA。血浆置换和类固醇治疗迅速启动,但溶血仍持续。进一步检查显示巨幼细胞贫血、严重维生素B12缺乏、高铁饱和度以及网织红细胞缺乏,这些均无法用TTP解释。严重维生素B12缺乏可导致骨髓中未能完成成熟过程的红细胞破坏而引起溶血性贫血。然而,这不应导致血栓性微血管病。先前关于维生素B12缺乏伴MAHA及TTP样表现的报道已确定急性高同型半胱氨酸血症是维生素B12缺乏与MAHA之间缺失的环节,因此进一步探讨了这种可能性。我们的患者同样血清同型半胱氨酸水平显著升高,证实了对维生素B12缺乏的怀疑。补充维生素B12使升高的同型半胱氨酸水平恢复正常,外周血涂片上裂体细胞消失,微血管病性溶血得到缓解,从而确诊。重症监护医生不仅要了解早期识别和治疗TTP的重要性,还应熟悉可能以类似方式出现的罕见病症,这一点至关重要。