Frasier Lane L, Azari David P, Ma Yue, Pavuluri Quamme Sudha R, Radwin Robert G, Pugh Carla M, Yen Thomas Y, Chen Chia-Hsiung, Greenberg Caprice C
Wisconsin Surgical Outcomes Research Program, Department of Surgery, University of Wisconsin-Madison, Madison, WI.
Department of Industrial and Systems Engineering, University of Wisconsin-Madison, Madison, WI.
Surgery. 2016 Nov;160(5):1400-1413. doi: 10.1016/j.surg.2016.05.004. Epub 2016 Jun 21.
Often in simulated settings, quantitative analysis of technical skill relies largely on specially tagged instruments or tracers on surgeons' hands. We investigated a novel, marker-less technique for evaluating technical skill during open operations and for differentiating tasks and surgeon experience level.
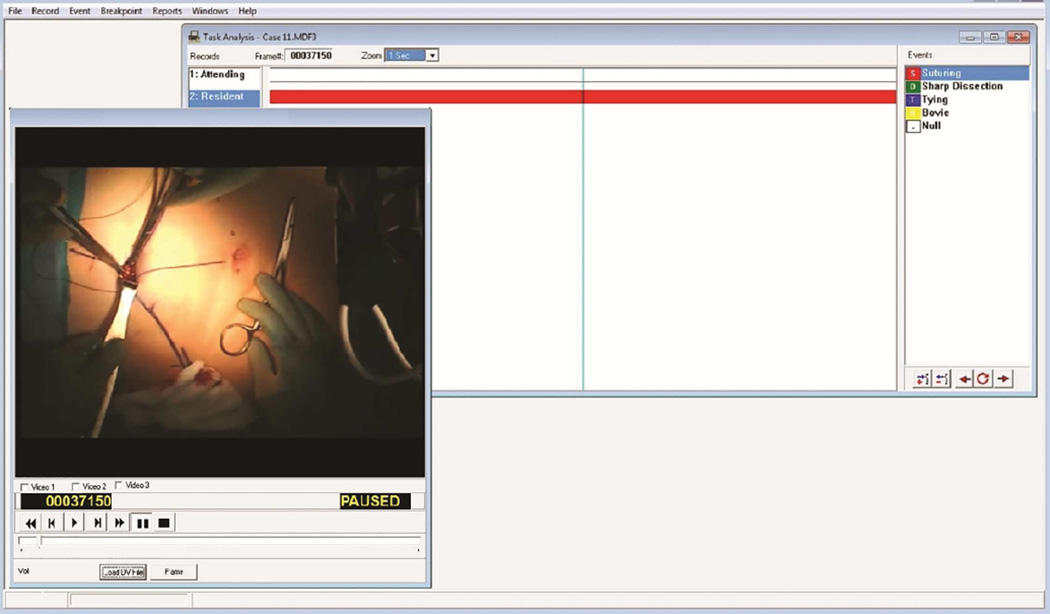
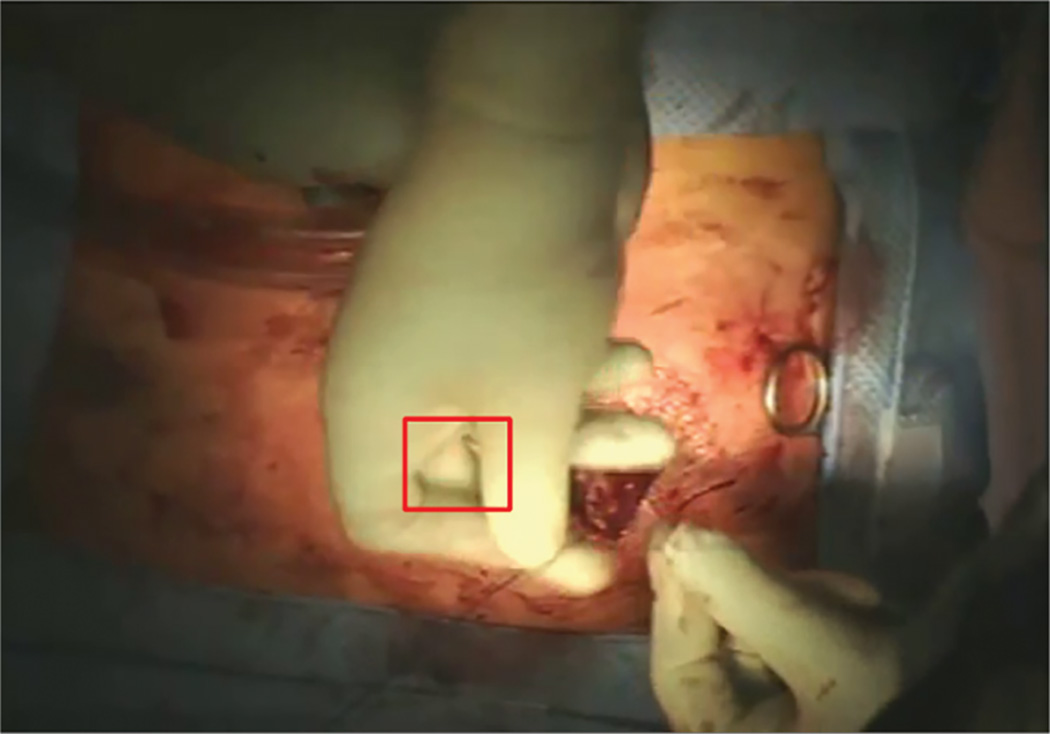
We recorded the operative field via in-light camera for open operations. Sixteen cases yielded 138 video clips of suturing and tying tasks ≥5 seconds in duration. Video clips were categorized based on surgeon role (attending, resident) and task subtype (suturing tasks: body wall, bowel anastomosis, complex anastomosis; tying tasks: body wall, superficial tying, deep tying). We tracked a region of interest on the hand to generate kinematic data. Nested, multilevel modeling addressed the nonindependence of clips obtained from the same surgeon.
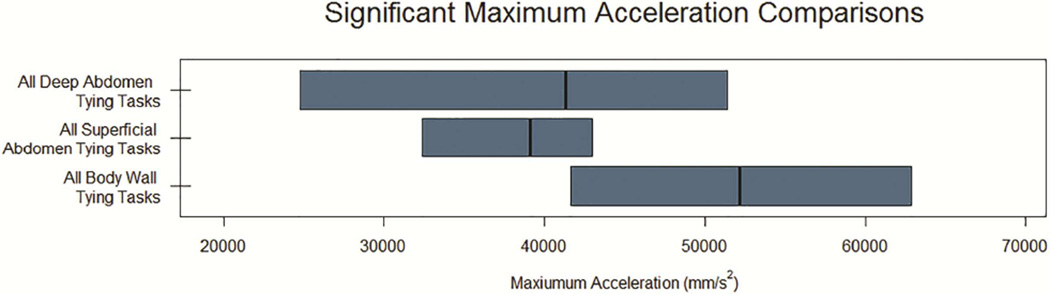
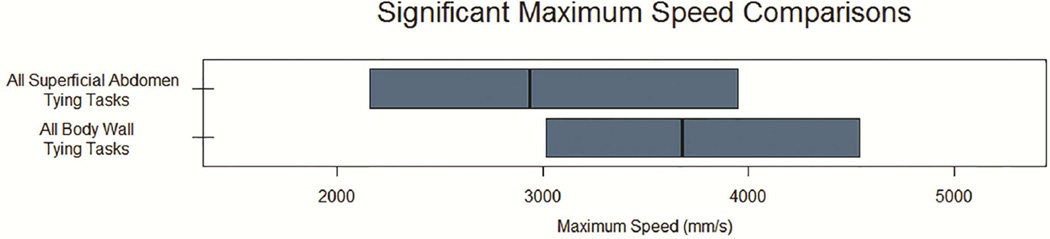
Interaction effects for suturing tasks were seen between role and task categories for average speed (P = .04), standard deviation of speed (P = .05), and average acceleration (P = .03). There were significant differences across task categories for standard deviation of acceleration (P = .02). Significant differences for tying tasks across task categories were observed for maximum speed (P = .02); standard deviation of speed (P = .04); and average (P = .02), maximum (P < .01), and standard deviation (P = .03) of acceleration.
We demonstrated the ability to detect kinematic differences in performance using marker-less tracking during open operative cases. Suturing task evaluation was most sensitive to differences in surgeon role and task category and may represent a scalable approach for providing quantitative feedback to surgeons about technical skill.
在模拟环境中,技术技能的定量分析很大程度上依赖于外科医生手上特别标记的器械或示踪剂。我们研究了一种新颖的、无标记技术,用于评估开放手术中的技术技能,并区分任务和外科医生的经验水平。
我们通过内置摄像头记录开放手术的术野。16个病例产生了138个持续时间≥5秒的缝合和打结任务视频片段。视频片段根据外科医生角色(主治医生、住院医生)和任务子类型(缝合任务:体壁、肠吻合、复杂吻合;打结任务:体壁、浅部打结、深部打结)进行分类。我们追踪手部的感兴趣区域以生成运动学数据。嵌套的多级建模解决了从同一位外科医生获得的片段之间的非独立性问题。
在缝合任务中,角色和任务类别之间在平均速度(P = 0.04)、速度标准差(P = 0.05)和平均加速度(P = 0.03)方面存在交互作用。在加速度标准差方面,各任务类别之间存在显著差异(P = 0.02)。在打结任务中,各任务类别在最大速度(P = 0.02)、速度标准差(P = 0.04)以及加速度的平均值(P = 0.02)、最大值(P < 0.01)和标准差(P = 0.03)方面存在显著差异。
我们证明了在开放手术病例中使用无标记跟踪检测性能运动学差异的能力。缝合任务评估对外科医生角色和任务类别的差异最为敏感,可能代表了一种可扩展的方法,用于向外科医生提供关于技术技能的定量反馈。