Finn Richard S, Crown John P, Ettl Johannes, Schmidt Marcus, Bondarenko Igor M, Lang Istvan, Pinter Tamas, Boer Katalin, Patel Ravindranath, Randolph Sophia, Kim Sindy T, Huang Xin, Schnell Patrick, Nadanaciva Sashi, Bartlett Cynthia Huang, Slamon Dennis J
Department of Medicine, Division of Hematology/Oncology, David Geffen School of Medicine at University of California Los Angeles, Los Angeles, CA, USA.
Irish Cooperative Oncology Research Group, Dublin, Ireland.
Breast Cancer Res. 2016 Jun 28;18(1):67. doi: 10.1186/s13058-016-0721-5.
Palbociclib is an oral small-molecule inhibitor of cyclin-dependent kinases 4 and 6. In the randomized, open-label, phase II PALOMA-1/TRIO-18 trial, palbociclib in combination with letrozole improved progression-free survival (PFS) compared with letrozole alone as first-line treatment of estrogen receptor (ER)-positive, human epidermal growth factor receptor 2 (HER2)-negative, advanced breast cancer (20.2 months versus 10.2 months; hazard ratio (HR) = 0.488, 95 % confidence interval (CI) 0.319-0.748; one-sided p = 0.0004). Grade 3-4 neutropenia was the most common adverse event (AE) in the palbociclib + letrozole arm. We now present efficacy and safety analyses based on several specific patient and tumor characteristics, and present in detail the clinical patterns of neutropenia observed in the palbociclib + letrozole arm of the overall safety population.
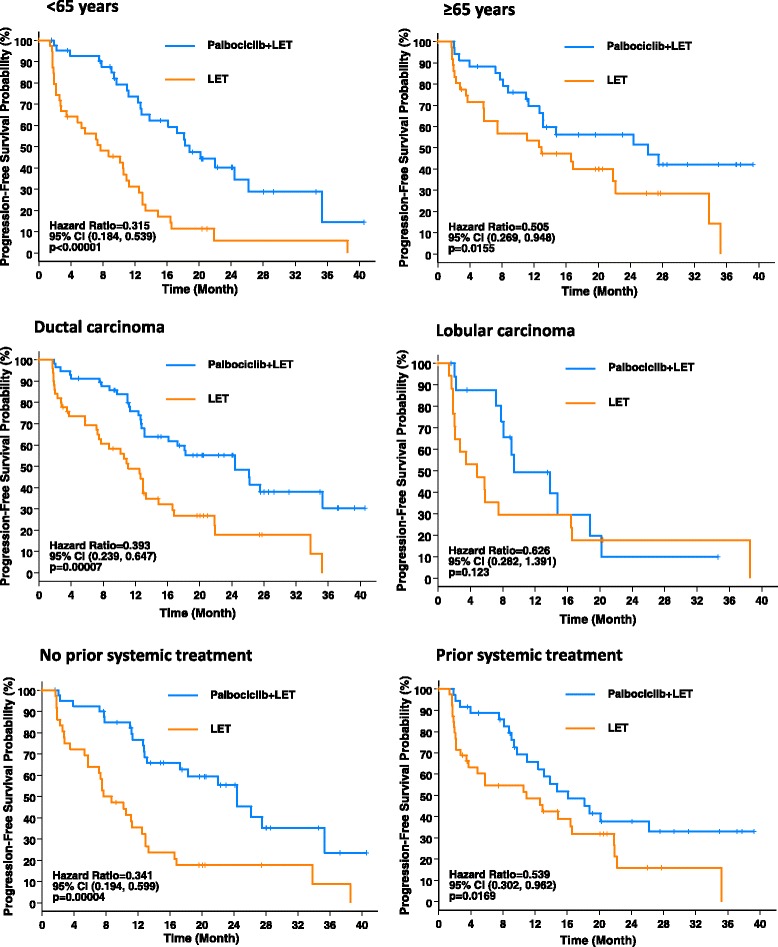
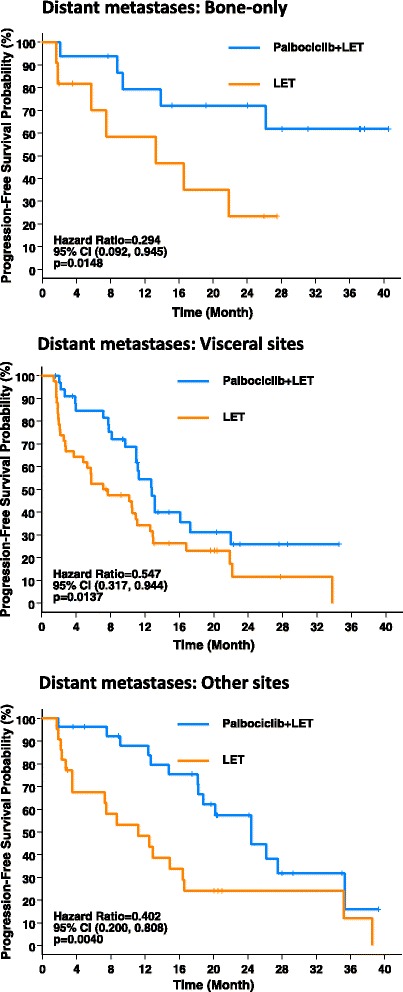
Postmenopausal women (n = 165) with ER+, HER2-negative, advanced breast cancer who had not received any systemic treatment for their advanced disease were randomized 1:1 to receive either palbociclib in combination with letrozole or letrozole alone. Treatment continued until disease progression, unacceptable toxicity, consent withdrawal, or death. The primary endpoint was PFS. We now analyze the difference in PFS for the treatment populations by subgroups, including age, histological type, history of prior neoadjuvant/adjuvant systemic treatment, and sites of distant metastasis, using the Kaplan-Meier method. HR and 95 % CI are derived from a Cox proportional hazards regression model.
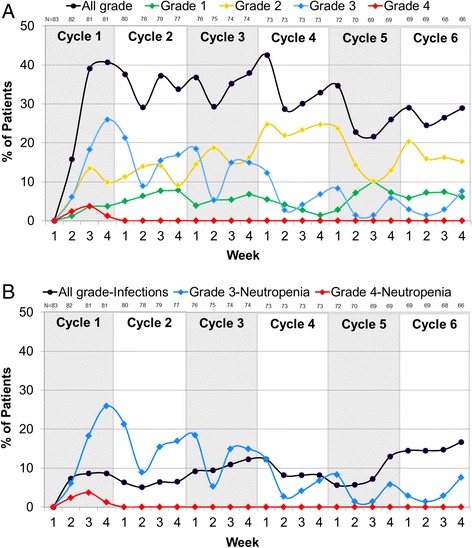
A clinically meaningful improvement in median PFS and clinical benefit response (CBR) rate was seen with palbociclib + letrozole in every subgroup evaluated. Grade 3-4 neutropenia was the most common AE with palbociclib + letrozole in all subgroups. Analysis of the frequency of neutropenia by grade during the first six cycles of treatment showed that there was a downward trend in Grade 3-4 neutropenia over time. Among those who experienced Grade 3-4 neutropenia, 71.7 % had no overlapping infections of any grade and none had overlapping Grade 3-4 infections.
The magnitude of clinical benefit seen with the addition of palbociclib to letrozole in improving both median PFS and CBR rate is consistent in nearly all subgroups analyzed, and consistent with that seen in the overall study population. The safety profile of the combination treatment in all subgroups was also comparable to that in the overall safety population of the study.
帕博西尼是一种细胞周期蛋白依赖性激酶4和6的口服小分子抑制剂。在随机、开放标签的II期PALOMA-1/TRIO-18试验中,与单独使用来曲唑作为雌激素受体(ER)阳性、人表皮生长因子受体2(HER2)阴性、晚期乳腺癌的一线治疗相比,帕博西尼联合来曲唑改善了无进展生存期(PFS)(20.2个月对10.2个月;风险比(HR)=0.488,95%置信区间(CI)0.319 - 0.748;单侧p = 0.0004)。3 - 4级中性粒细胞减少是帕博西尼 + 来曲唑组中最常见的不良事件(AE)。我们现在基于几种特定的患者和肿瘤特征进行疗效和安全性分析,并详细呈现总体安全人群中帕博西尼 + 来曲唑组观察到的中性粒细胞减少的临床模式。
165名未接受过晚期疾病全身治疗的绝经后ER +、HER2阴性晚期乳腺癌女性患者按1:1随机分组,分别接受帕博西尼联合来曲唑或单独使用来曲唑治疗。治疗持续至疾病进展、出现不可接受的毒性、患者撤回同意或死亡。主要终点是PFS。我们现在使用Kaplan-Meier方法分析各亚组(包括年龄、组织学类型、新辅助/辅助全身治疗史以及远处转移部位)治疗人群的PFS差异。HR和95%CI来自Cox比例风险回归模型。
在每个评估的亚组中,帕博西尼 + 来曲唑均使中位PFS和临床获益反应(CBR)率有临床意义的改善。3 - 4级中性粒细胞减少是所有亚组中帕博西尼 + 来曲唑最常见的AE。对治疗前六个周期中性粒细胞减少按等级的频率分析表明,3 - 4级中性粒细胞减少随时间呈下降趋势。在经历3 - 4级中性粒细胞减少的患者中,71.7%没有任何等级的重叠感染,且无一例有3 - 4级重叠感染。
在几乎所有分析的亚组中,帕博西尼联合来曲唑在改善中位PFS和CBR率方面的临床获益程度是一致的,且与总体研究人群中的情况一致。所有亚组中联合治疗的安全性概况也与研究总体安全人群中的情况相当。