Knight Elizabeth P, Shea Kimberly, Rosenfeld Anne G, Schmiege Sarah, Hsu Chiu-Hsieh, DeVon Holli A
Elizabeth P. Knight, DNP, PhD, RN,is Clinical Assistant Professor; Kimberly Shea, PhD, RN, is Clinical Associate Professor; and Anne G. Rosenfeld, PhD, RN, FAHA, FAAN, is Professor, College of Nursing, University of Arizona, Tucson. Sarah Schmiege, PhD, is Assistant Professor, University of Colorado-Denver College of Nursing. Chiu-Hsieh Hsu, PhD, is Associate Professor, University of Arizona College of Public Health, Tucson. Holli A. DeVon, PhD, RN, FAHA, FAAN, is Associate Professor, University of Illinois at Chicago College of Nursing.
Nurs Res. 2016 Jul-Aug;65(4):268-78. doi: 10.1097/NNR.0000000000000167.
Many patients evaluated for acute coronary syndrome (ACS) in emergency departments (EDs) continue to experience troubling symptoms after discharge-regardless of their ultimate medical diagnosis. However, comprehensive understanding of common post-ED symptom trajectories is lacking.
The aim of this study was to identify common trajectories of symptom severity in the 6 months after an ED visit for potential ACS.
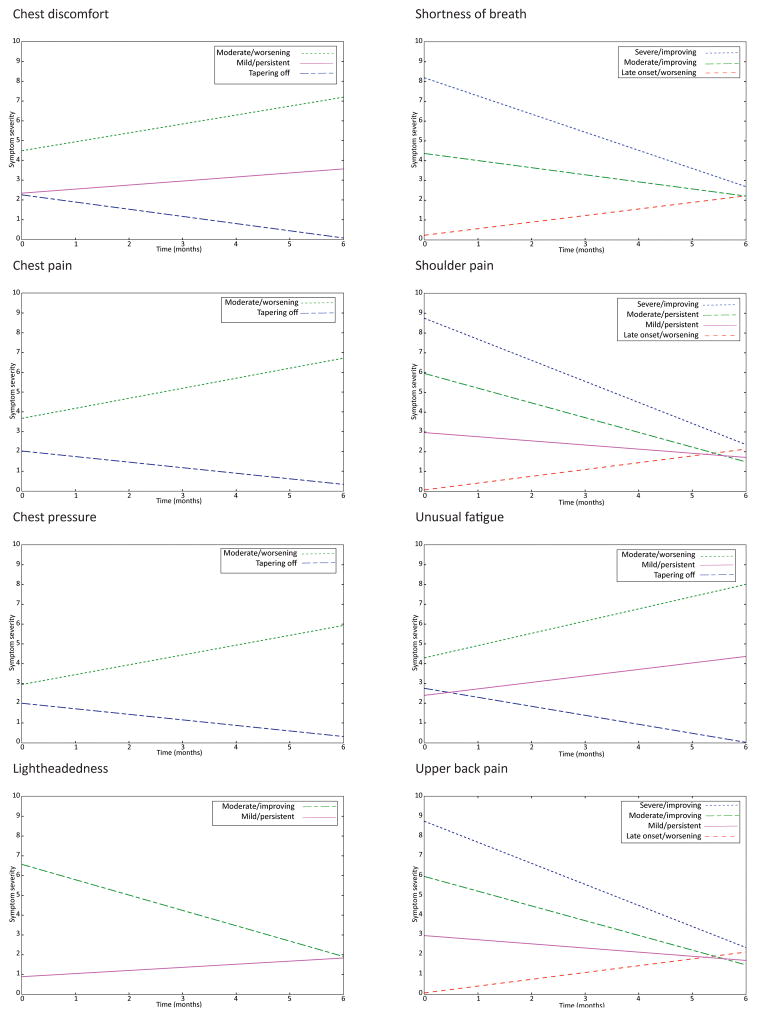
This was a secondary analysis of data from a larger observational, prospective study conducted in five U.S. EDs. Patients (N = 1005) who had electrocardiogram and biomarker testing ordered, and were identified by the triage nurse as potentially having ACS, were enrolled. Symptom severity was assessed in the hospital after initial stabilization and by telephone at 30 days and 6 months using the validated 13-item ACS Symptom Checklist. Growth mixture modeling was used for the secondary analysis. The eight most commonly reported symptoms (chest discomfort, chest pain, chest pressure, light-headedness, shortness of breath, shoulder pain, unusual fatigue, and upper back pain) were modeled across the three study time points. Models with increasing numbers of classes were compared, and final model selection was based on a combination of interpretability, theoretical justification, and statistical fit indices.
The sample was 62.6% male with a mean age of 60.2 years (SD = 14.17 years), and 57.1% ruled out for ACS. Between two and four distinct trajectory classes were identified for each symptom. The seven different types of trajectories identified across the eight symptoms were labeled "tapering off," "mild/persistent," "moderate/persistent," "moderate/worsening," "moderate/improving," "late onset, "and "severe/improving." Trajectories differed on age, gender, and diagnosis.
Research on the individual nature of symptom trajectories can contribute to patient-centered, rather than disease-centered, care. Further research is needed to verify the existence of multiple symptoms trajectories in diverse populations and to assess the antecedents and consequences of individual symptom trajectories.
许多在急诊科(ED)接受急性冠状动脉综合征(ACS)评估的患者出院后仍有令人困扰的症状——无论其最终的医学诊断如何。然而,目前缺乏对急诊科后常见症状轨迹的全面了解。
本研究的目的是确定因疑似ACS到急诊科就诊后6个月内症状严重程度的常见轨迹。
这是对在美国5个急诊科进行的一项更大规模的观察性前瞻性研究数据的二次分析。纳入了接受心电图和生物标志物检测、且被分诊护士确定可能患有ACS的患者(N = 1005)。在初始稳定后于医院内评估症状严重程度,并在30天和6个月时通过电话使用经过验证的13项ACS症状清单进行评估。二次分析采用生长混合模型。对三个研究时间点的八种最常报告的症状(胸部不适、胸痛、胸部压迫感、头晕、呼吸急促、肩部疼痛、异常疲劳和上背部疼痛)进行建模。比较了不同类别数量的模型,最终模型选择基于可解释性、理论依据和统计拟合指数的综合考虑。
样本中男性占62.6%,平均年龄为60.2岁(标准差 = 14.17岁),57.1%的患者排除了ACS。每种症状确定了两到四个不同的轨迹类别。在八种症状中确定的七种不同类型的轨迹分别标记为“逐渐减轻”、“轻度/持续”、“中度/持续”、“中度/恶化”、“中度/改善”、“延迟发作”和“重度/改善”。轨迹在年龄、性别和诊断方面存在差异。
对症状轨迹个体性质的研究有助于以患者为中心而非以疾病为中心的护理。需要进一步研究以验证不同人群中多种症状轨迹的存在,并评估个体症状轨迹的前因后果。