Tabarestani Sanaz, Movafagh Abolfazl
Cancer Research Center, Shahid Beheshti University of Medical Sciences, Tehran, IR Iran.
Medical Genetics Department, Faculty of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, IR Iran.
Iran J Cancer Prev. 2016 Feb 22;9(1):e3961. doi: 10.17795/ijcp-3961. eCollection 2016 Feb.
Chronic myeloid leukemia (CML) is a myeloproliferative disorder characterized by overproduction of immature and matured myeloid cells in the peripheral blood, bone marrow and spleen.
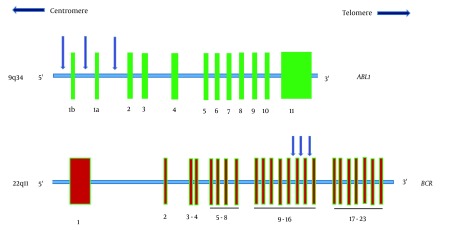
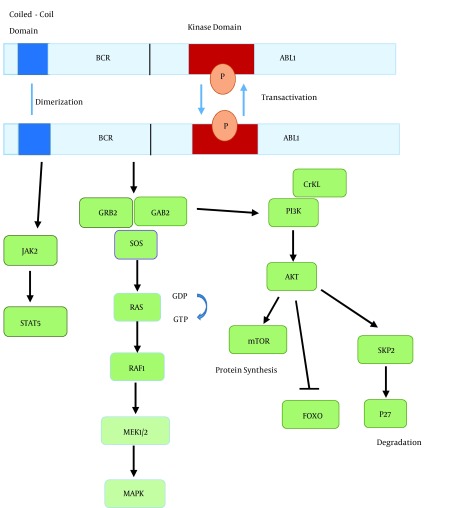
A hallmark of CML is the presence of (9; 22) (q34; q11) reciprocal translocation, which is cytogenetically visible as Philadelphia chromosome (Ph) and results in the formation of BCR-ABL1 fusion protein. This fusion protein is a constitutively active tyrosine kinase which is necessary and sufficient for malignant transformation. The introduction of imatinib, a BCR-ABL1- targeting tyrosine kinase inhibitor (TKI) has revolutionized CML therapy. Subsequently, two other TKIs with increased activity against BCR-ABL1, dasatinib and nilotinib, were developed and approved for CML patients. Nevertheless, CML therapy faces major challenges.
The first is the development of resistance to BCR-ABL1 inhibitors in some patients, which can be due to BCR-ABL1 overexpression, differences in cellular drug influx and efflux, activation of alternative signaling pathways, or emergence of BCR-ABL1 kinase domain mutations during TKI treatment. The second is the limited efficiency of BCR-ABL1-TKIs in blast crisis (BC) CML. The third is the insensitivity of CML stem cells to BCR-ABL1 inhibitors. Conventional chemotherapeutics and BCR-ABL1 inhibitors which act by inhibiting cell proliferation and inducing apoptosis, are ineffective against quiescent CML stem cells.
A better understanding of the mechanisms that underlie TKI resistance, progression to BC, genomic instability and stem cell quiescence is essential to develop curative strategies for patients with CML.
慢性髓性白血病(CML)是一种骨髓增殖性疾病,其特征是外周血、骨髓和脾脏中未成熟和成熟髓细胞过度生成。
CML的一个标志是存在(9;22)(q34;q11)相互易位,在细胞遗传学上可见为费城染色体(Ph),并导致BCR-ABL1融合蛋白的形成。这种融合蛋白是一种组成型活性酪氨酸激酶,对恶性转化是必需且充分的。伊马替尼(一种靶向BCR-ABL1的酪氨酸激酶抑制剂(TKI))的引入彻底改变了CML的治疗方法。随后,另外两种对BCR-ABL1活性增强的TKI(达沙替尼和尼罗替尼)被开发并批准用于CML患者。然而,CML治疗面临重大挑战。
首先,一些患者会对BCR-ABL1抑制剂产生耐药性,这可能是由于BCR-ABL1过表达、细胞药物流入和流出的差异、替代信号通路的激活,或在TKI治疗期间BCR-ABL1激酶结构域突变的出现。其次,BCR-ABL1-TKIs在急变期(BC)CML中的疗效有限。第三,CML干细胞对BCR-ABL1抑制剂不敏感。通过抑制细胞增殖和诱导凋亡起作用的传统化疗药物和BCR-ABL1抑制剂对静止的CML干细胞无效。
更好地理解TKI耐药、进展为BC、基因组不稳定和干细胞静止的潜在机制对于为CML患者制定治愈策略至关重要。