Dominguez Fernando, Ramos Antonio, Bouza Emilio, Muñoz Patricia, Valerio Maricela C, Fariñas M Carmen, de Berrazueta José Ramón, Zarauza Jesús, Pericás Pulido Juan Manuel, Paré Juan Carlos, de Alarcón Arístides, Sousa Dolores, Rodriguez Bailón Isabel, Montejo-Baranda Miguel, Noureddine Mariam, García Vázquez Elisa, Garcia-Pavia Pablo
aDepartment of Cardiology, Heart Failure and Inherited Cardiac Diseases Unit, Hospital Universitario Puerta de Hierro bInfectious Diseases Unit, Department of Internal Medicine, Hospital Universitario Puerta de Hierro cClinical Microbiology and Infectious Diseases Unit, Hospital General Universitario Gregorio Marañón dHealth Research Institute Gregorio Marañón, CIBER Respiratory Diseases-CIBERES (CB06/06/0058), Medical School, Complutense University, Madrid eInfectious Diseases Unit, Hospital Universitario Marqués de Valdecilla fDepartment of Cardiology, Hospital Universitario Marqués de Valdecilla gDepartment of Cardiology, Hospital de Sierrallana, Santander hInfectious Diseases Unit, Hospital Clinic-IDIBAPS, Barcelona University iDepartment of Cardiology, Hospital Clinic-IDIBAPS, Barcelona University, Barcelona jDepartment of Infectious Diseases, Hospital Universitario Virgen del Rocío, Seville kInfectious Diseases Unit, Complejo Hospitalario Universitario A Coruña, A Coruña lDepartment of Cardiology, Hospital Virgen de la Victoria, Málaga mInfectious Diseases Unit, Hospital Universitario Cruces, País Vasco University, Bilbao nDepartment of Internal Medicine, Hospital Costa del Sol, Marbella, Málaga oDepartment of Internal Medicine-Infectious Diseases, Hospital Universitario Virgen de la Arrixaca, Medical School, Murcia University, Murcia pMyocardial Biology Programme, Centro Nacional de Investigaciones Cardiovasculares (CNIC), Madrid, Spain.
Medicine (Baltimore). 2016 Jun;95(26):e4008. doi: 10.1097/MD.0000000000004008.
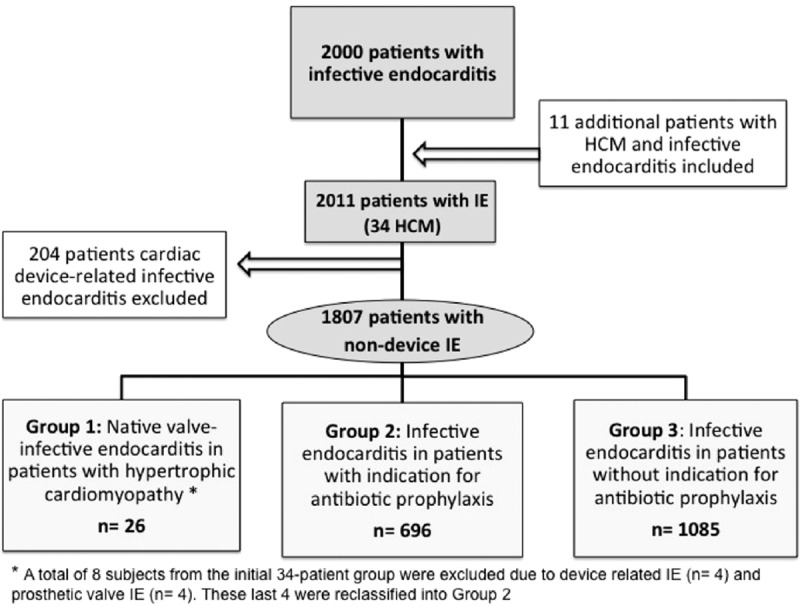
Infective endocarditis (IE) complicating hypertrophic cardiomyopathy (HCM) is a poorly known entity. Although current guidelines do not recommend IE antibiotic prophylaxis (IEAP) in HCM, controversy remains.This study sought to describe the clinical course of a large series of IE HCM and to compare IE in HCM patients with IE patients with and without an indication for IEAP.Data from the GAMES IE registry involving 27 Spanish hospitals were analyzed. From January 2008 to December 2013, 2000 consecutive IE patients were prospectively included in the registry. Eleven IE HCM additional cases from before 2008 were also studied. Clinical, microbiological, and echocardiographic characteristics were analyzed in IE HCM patients (n = 34) and in IE HCM reported in literature (n = 84). Patients with nondevice IE (n = 1807) were classified into 3 groups: group 1, HCM with native-valve IE (n = 26); group 2, patients with IEAP indication (n = 696); group 3, patients with no IEAP indication (n = 1085). IE episode and 1-year follow-up data were gathered.One-year mortality in IE HCM was 42% in our study and 22% in the literature. IE was more frequent, although not exclusive, in obstructive HCM (59% and 74%, respectively). Group 1 exhibited more IE predisposing factors than groups 2 and 3 (62% vs 40% vs 50%, P < 0.01), and more previous dental procedures (23% vs 6% vs 8%, P < 0.01). Furthermore, Group 1 experienced a higher incidence of Streptococcus infections than Group 2 (39% vs 22%, P < 0.01) and similar to Group 3 (39% vs 30%, P = 0.34). Overall mortality was similar among groups (42% vs 36% vs 35%, P = 0.64).IE occurs in HCM patients with and without obstruction. Mortality of IE HCM is high but similar to patients with and without IEAP indication. Predisposing factors, previous dental procedures, and streptococcal infection are higher in IE HCM, suggesting that HCM patients could benefit from IEAP.
感染性心内膜炎(IE)并发肥厚型心肌病(HCM)是一种鲜为人知的疾病。尽管当前指南不推荐对肥厚型心肌病患者进行感染性心内膜炎抗生素预防(IEAP),但争议仍然存在。本研究旨在描述一系列大量肥厚型心肌病合并感染性心内膜炎患者的临床病程,并比较有IEAP指征和无IEAP指征的肥厚型心肌病患者与感染性心内膜炎患者的情况。分析了来自西班牙27家医院的GAMES IE注册研究的数据。2008年1月至2013年12月,共有2000例连续的感染性心内膜炎患者被前瞻性纳入该注册研究。还研究了2008年之前的11例肥厚型心肌病合并感染性心内膜炎的额外病例。分析了肥厚型心肌病合并感染性心内膜炎患者(n = 34)和文献报道的肥厚型心肌病合并感染性心内膜炎患者(n = 84)的临床、微生物学和超声心动图特征。非器械相关感染性心内膜炎患者(n = 1807)分为3组:第1组,肥厚型心肌病合并天然瓣膜感染性心内膜炎(n = 26);第2组,有IEAP指征的患者(n = 696);第3组,无IEAP指征的患者(n = 1085)。收集了感染性心内膜炎发作和1年随访数据。在我们的研究中,肥厚型心肌病合并感染性心内膜炎患者的1年死亡率为42%,文献报道为22%。感染性心内膜炎在梗阻性肥厚型心肌病中更常见,尽管并非唯一(分别为59%和74%)。第1组比第2组和第3组表现出更多的感染性心内膜炎易感因素(62%对40%对50%,P<0.01),并且有更多的既往牙科手术史(23%对6%对8%,P<0.01)。此外,第1组链球菌感染的发生率高于第2组(39%对22%,P<0.01),与第3组相似(39%对30%,P = 0.34)。各组总体死亡率相似(42%对36%对35%,P = 0.64)。
感染性心内膜炎可发生于有或无梗阻的肥厚型心肌病患者。肥厚型心肌病合并感染性心内膜炎的死亡率很高,但与有或无IEAP指征的患者相似。肥厚型心肌病合并感染性心内膜炎的易感因素、既往牙科手术史和链球菌感染率更高,这表明肥厚型心肌病患者可能从IEAP中获益。