Chitty Lyn S, Wright David, Hill Melissa, Verhoef Talitha I, Daley Rebecca, Lewis Celine, Mason Sarah, McKay Fiona, Jenkins Lucy, Howarth Abigail, Cameron Louise, McEwan Alec, Fisher Jane, Kroese Mark, Morris Stephen
Genetics and Genomic Medicine, UCL Institute of Child Health, London WC1N 3BH, UK Great Ormond Street Hospital for Children NHS Foundation Trust, London, UK.
Department of Statistics, Plymouth University, Plymouth, UK.
BMJ. 2016 Jul 4;354:i3426. doi: 10.1136/bmj.i3426.
To investigate the benefits and costs of implementing non-invasive prenatal testing (NIPT) for Down's syndrome into the NHS maternity care pathway.
Prospective cohort study.
Eight maternity units across the United Kingdom between 1 November 2013 and 28 February 2015.
All pregnant women with a current Down's syndrome risk on screening of at least 1/1000.
Outcomes were uptake of NIPT, number of cases of Down's syndrome detected, invasive tests performed, and miscarriages avoided. Pregnancy outcomes and costs associated with implementation of NIPT, compared with current screening, were determined using study data on NIPT uptake and invasive testing in combination with national datasets.
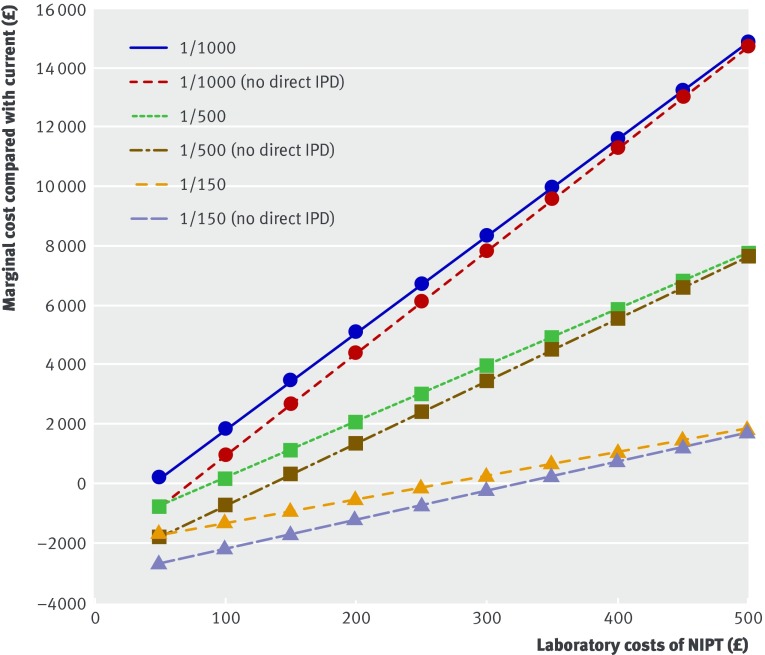
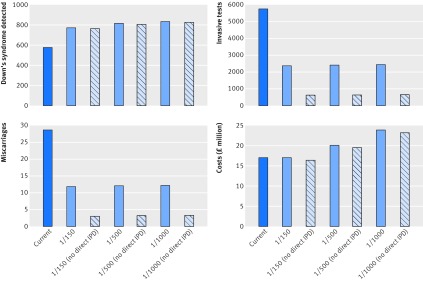
NIPT was prospectively offered to 3175 pregnant women. In 934 women with a Down's syndrome risk greater than 1/150, 695 (74.4%) chose NIPT, 166 (17.8%) chose invasive testing, and 73 (7.8%) declined further testing. Of 2241 women with risks between 1/151 and 1/1000, 1799 (80.3%) chose NIPT. Of 71 pregnancies with a confirmed diagnosis of Down's syndrome, 13/42 (31%) with the diagnosis after NIPT and 2/29 (7%) after direct invasive testing continued, resulting in 12 live births. In an annual screening population of 698 500, offering NIPT as a contingent test to women with a Down's syndrome screening risk of at least 1/150 would increase detection by 195 (95% uncertainty interval -34 to 480) cases with 3368 (2279 to 4027) fewer invasive tests and 17 (7 to 30) fewer procedure related miscarriages, for a non-significant difference in total costs (£-46 000, £-1 802 000 to £2 661 000). The marginal cost of NIPT testing strategies versus current screening is very sensitive to NIPT costs; at a screening threshold of 1/150, NIPT would be cheaper than current screening if it cost less than £256. Lowering the risk threshold increases the number of Down's syndrome cases detected and overall costs, while maintaining the reduction in invasive tests and procedure related miscarriages.
Implementation of NIPT as a contingent test within a public sector Down's syndrome screening programme can improve quality of care, choices for women, and overall performance within the current budget. As some women use NIPT for information only, the Down's syndrome live birth rate may not change significantly. Future research should consider NIPT uptake and informed decision making outside of a research setting.
探讨在英国国民医疗服务体系(NHS)产科护理路径中实施唐氏综合征无创产前检测(NIPT)的益处和成本。
前瞻性队列研究。
2013年11月1日至2015年2月28日期间英国的8个产科单位。
所有筛查时唐氏综合征风险至少为1/1000的孕妇。
NIPT的接受情况、检测出的唐氏综合征病例数、进行的侵入性检测以及避免的流产情况。与当前筛查相比,使用关于NIPT接受情况和侵入性检测的研究数据以及国家数据集来确定与实施NIPT相关的妊娠结局和成本。
前瞻性地为3175名孕妇提供了NIPT。在934名唐氏综合征风险大于1/150的女性中,695名(74.4%)选择了NIPT,166名(17.8%)选择了侵入性检测,73名(7.8%)拒绝进一步检测。在2241名风险在1/151至1/1000之间的女性中,1799名(80.3%)选择了NIPT。在71例确诊为唐氏综合征的妊娠中,42例经NIPT诊断后有13例(31%)继续妊娠,29例直接经侵入性检测诊断后有2例(7%)继续妊娠,共12例活产。在每年698500人的筛查人群中,将NIPT作为应急检测提供给唐氏综合征筛查风险至少为1/150的女性,可增加195例(95%不确定区间 -34至480)的检测病例数,减少3368例(2279至4027)侵入性检测,减少17例(7至30)与操作相关的流产,总成本差异无统计学意义(-46000英镑,-1802000至2661000英镑)。与当前筛查相比,NIPT检测策略的边际成本对NIPT成本非常敏感;在筛查阈值为1/150时,如果NIPT成本低于256英镑,其将比当前筛查更便宜。降低风险阈值会增加检测出的唐氏综合征病例数和总体成本,同时保持侵入性检测和与操作相关流产的减少。
在公共部门唐氏综合征筛查项目中实施NIPT作为应急检测可以提高护理质量、为女性提供更多选择,并在当前预算范围内改善整体绩效。由于一些女性仅将NIPT用于获取信息,唐氏综合征活产率可能不会有显著变化。未来的研究应考虑在研究环境之外的NIPT接受情况和知情决策。