de Souza Ana Luiza Ribeiro, Marra Kayla, Gunn Jason, Samkoe Kimberley S, Hoopes P Jack, Feldwisch Joachim, Paulsen Keith D, Pogue Brian W
Thayer School of Engineering, Dartmouth College, 14 Engineering Drive, Hanover, NH, 03755, USA.
CAPES Foundation, Ministry of Education of Brazil, Brasilia, DF, 70040-020, Brazil.
Mol Imaging Biol. 2017 Feb;19(1):41-48. doi: 10.1007/s11307-016-0980-7.
Fluorescence guidance in surgical oncology provides the potential to realize enhanced molecular tumor contrast with dedicated targeted tracers, potentially with a microdose injection level. For most glioma tumors, the blood brain barrier is compromised allowing some exogenous drug/molecule delivery and accumulation for imaging. The aberrant overexpression and/or activation of epidermal growth factor receptor (EGFR) is associated with many types of cancers, including glioblastoma, and so the use of a near-infrared (NIR) fluorescent molecule targeted to the EGFR receptor provides the potential for improving tumor contrast during surgery. Fluorescently labeled affibody molecule (ABY-029) has high EGFR affinity and high potential specificity with reasonably fast plasma clearance. In this study, ABY-29 was evaluated in glioma versus normal brain uptake from intravenous injection at a range of doses, down to a microdose injection level.
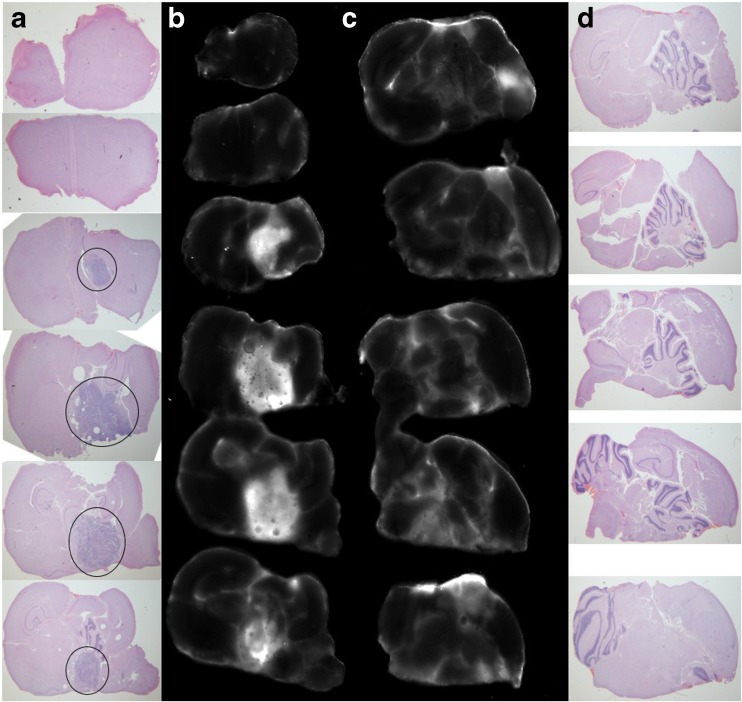
Nude rats were inoculated with the U251 human glioma cell line in the brain. Tumors were allowed to grow for 3-4 weeks. ABY-029 fluorescence ex vivo imaging of brain slices was acquired at different time points (1-48 h) and varying injection doses from 25 to 122 μg/kg (from human protein microdose equivalent to five times microdose levels).
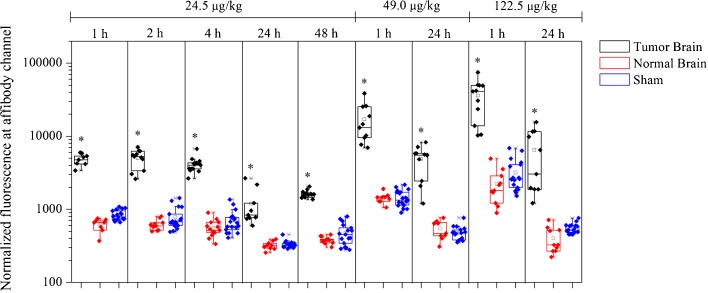
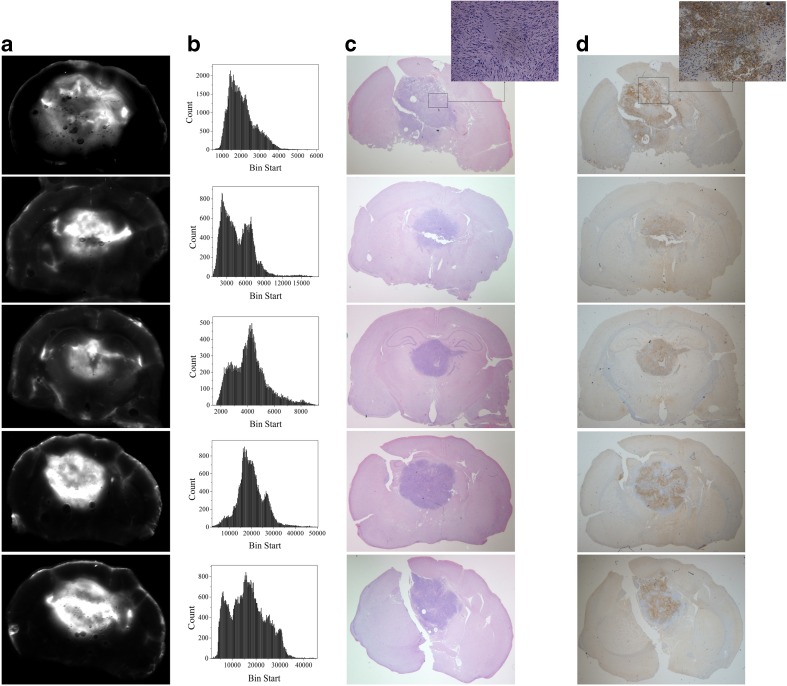
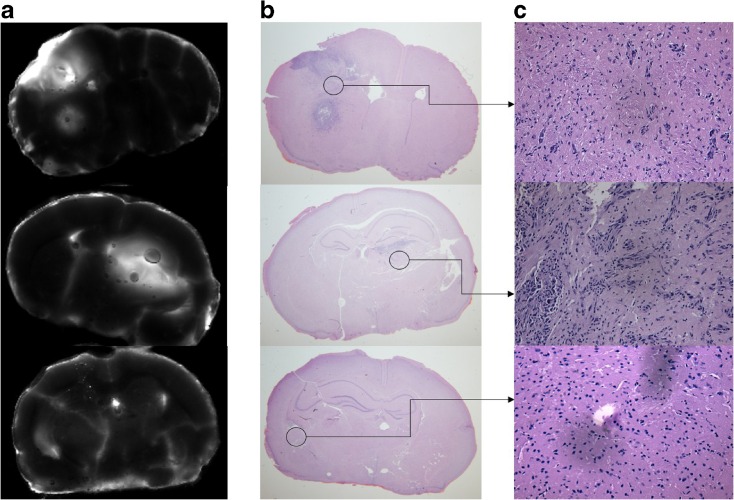
The tumor was most clearly visualized at 1-h post-injection with 8- to 16-fold average contrast relative to normal brain. However, the tumor still could be identified after 48 h. In all cases, the ABY-029 fluorescence appeared to localize preferentially in EGFR-positive regions. Increasing the injected dose from a microdose level to five times, a microdose level increased the signal by 10-fold, and the contrast was from 8 to 16, showing that there was value in doses slightly higher than the microdose restriction. Normal tissue uptake was found to be affected by the tumor size, indicating that edema was a likely factor affecting the expected tumor to normal tissue contrast.
These results suggest that the NIR-labeled affibody molecules provide an excellent potential to increase surgical visualization of EGFR-positive tumor regions.
外科肿瘤学中的荧光引导技术有潜力通过专用的靶向示踪剂实现增强的分子肿瘤对比度,可能只需微量注射水平。对于大多数胶质瘤肿瘤,血脑屏障受损,允许一些外源性药物/分子递送并积累用于成像。表皮生长因子受体(EGFR)的异常过表达和/或激活与多种癌症相关,包括胶质母细胞瘤,因此使用靶向EGFR受体的近红外(NIR)荧光分子有潜力在手术期间改善肿瘤对比度。荧光标记的亲和体分子(ABY - 029)具有高EGFR亲和力和高潜在特异性,且血浆清除速度合理。在本研究中,对ABY - 29在胶质瘤与正常脑内静脉注射不同剂量直至微量注射水平时的摄取情况进行了评估。
将U251人胶质瘤细胞系接种到裸鼠脑内。使肿瘤生长3 - 4周。在不同时间点(1 - 48小时)和从25至122μg/kg(从人蛋白微量等效剂量到五倍微量水平)的不同注射剂量下,获取脑切片的ABY - 029荧光离体成像。
注射后1小时肿瘤可视化最清晰,相对于正常脑平均对比度为8至16倍。然而,48小时后肿瘤仍可识别。在所有情况下,ABY - 029荧光似乎优先定位于EGFR阳性区域。将注射剂量从微量水平增加到五倍微量水平,信号增强了10倍,对比度从8增加到16,表明略高于微量限制的剂量是有价值的。发现正常组织摄取受肿瘤大小影响,表明水肿可能是影响预期肿瘤与正常组织对比度的一个因素。
这些结果表明,近红外标记的亲和体分子有极大潜力增强EGFR阳性肿瘤区域的手术可视化。