Shultz Blake, Timek Tomasz, Davis Alan T, Heiser John, Murphy Edward, Willekes Charles, Hooker Robert
Department of Thoracic and Cardiovascular Surgery, Spectrum Health, Fred and Lena Meijer Heart and Vascular Institute, 100 Michigan St. NE, 49503, Grand Rapids, MI, USA.
, 123 York Street Apt. #22V, New Haven, CT, 06511, USA.
J Cardiothorac Surg. 2016 Jul 12;11(1):105. doi: 10.1186/s13019-016-0501-4.
Long cross clamp times have been associated with poor clinical outcomes, yet some patients require extremely long ischemic times to repair complex surgical problems. The purpose of this study was to examine short and mid-term survival and to identify risk factors for mortality and morbidity in patients with cross clamp times greater than or equal to 300 min.
Review of our institution's Society of Thoracic Surgeons database identified 202 patients who underwent surgical procedures necessitating aortic cross clamp times 300 min or greater between 2001 and 2012. Short-term (30-day) clinical outcomes were derived from this database and survival was assessed utilizing the Social Security Death Index. Univariate and multivariate analyses were used to determine the relationship between independent variables and mortality and postoperative outcomes.
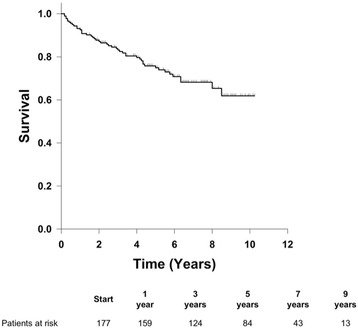
The average age of the patients was 69.5 ± 10.6 (mean ± standard deviation) years and the mean ejection fraction was 52 ± 12 %. 70.3 % of patients were male. Mean cross clamp time was 346 ± 45 min, and total bypass time was 421 ± 70 min. Thirty-day mortality was 12.4 %. The incidence of bleeding and stroke were 6.4 % and 4.0 % respectively. Prolonged ventilation occurred in 26.7 % of patients, and incidence of renal failure was 10.4 %. One, three, five, and seven year survival of the patients who survived the first 30 days post-surgery was 91.9 %, 83.2 %, 75.6 % and 65.7 % respectively. Proportional hazards analysis determined that the statistically significant hazard ratios for mid-term mortality for female gender, age, and prolonged postoperative ventilation were 2.11, 1.04 and 2.72, respectively (p < 0.05 for each).
Cardiac procedures requiring extremely long ischemic times have significant early mortality and morbidity. However, mid-term survival in the patients who survive is good. Decision-making regarding operability in complex cases should allow for long ischemic times.
较长的主动脉阻断时间与不良临床结局相关,但一些患者需要极长的缺血时间来修复复杂的外科问题。本研究的目的是检查短期和中期生存率,并确定主动脉阻断时间大于或等于300分钟的患者的死亡和发病风险因素。
回顾我们机构的胸外科医师协会数据库,确定了202例在2001年至2012年间接受手术且主动脉阻断时间达300分钟或更长时间的患者。短期(30天)临床结局来自该数据库,并利用社会保障死亡指数评估生存率。采用单因素和多因素分析来确定自变量与死亡率及术后结局之间的关系。
患者的平均年龄为69.5±10.6(均值±标准差)岁,平均射血分数为52±12%。70.3%的患者为男性。平均主动脉阻断时间为346±45分钟,总体外循环时间为421±70分钟。30天死亡率为12.4%。出血和中风的发生率分别为6.4%和4.0%。26.7%的患者出现通气时间延长,肾衰竭发生率为10.4%。术后存活30天的患者1年、3年、5年和7年生存率分别为91.9%、83.2%、75.6%和65.7%。比例风险分析确定,女性、年龄和术后通气时间延长的中期死亡风险比具有统计学意义,分别为2.11、1.04和2.72(各p<0.05)。
需要极长缺血时间的心脏手术有显著的早期死亡率和发病率。然而,存活患者的中期生存率良好。复杂病例中关于手术可行性的决策应考虑到较长的缺血时间。