Shewale Anand, Johnson Jill, Li Chenghui, Nelsen David, Martin Bradley
Division of Pharmaceutical Evaluation and Policy, University of Arkansas for Medical Sciences, Little Rock, AR 72205, USA.
Department of Pharmacy Practice, University of Arkansas for Medical Sciences, Little Rock, AR 72205, USA.
Healthcare (Basel). 2015 Mar 5;3(1):130-45. doi: 10.3390/healthcare3010130.
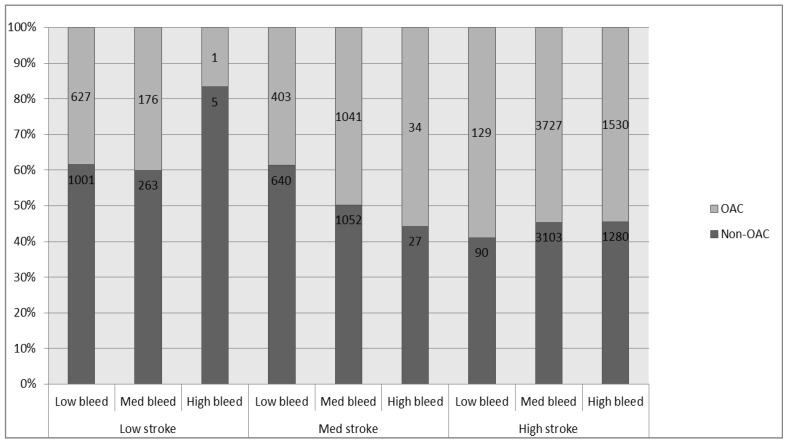
Published atrial fibrillation (AF) guidelines and decision tools offer oral anticoagulant (OAC) recommendations; however, they consider stroke and bleeding risk differently. The aims of our study are: (i) to compare the variation in OAC recommendations by the 2012 American College of Chest Physicians guidelines, the 2012 European Society of Cardiology (ESC) guidelines, the 2014 American Heart Association (AHA) guidelines and two published decision tools by Casciano and LaHaye; (ii) to compare the concordance with actual OAC use in the overall study population and the population stratified by stroke/bleed risk. A cross-sectional study using the 2001-2013 Lifelink claims data was used to contrast the treatment recommendations by these decision aids. CHA₂DS₂-VASc and HAS-BLED algorithms were used to stratify 15,129 AF patients into nine stroke/bleed risk groups to study the variation in treatment recommendations and concordance with actual OAC use/non-use. The AHA guidelines which were set to recommend OAC when CHA₂DS₂-VASc = 1 recommended OAC most often (86.30%) and the LaHaye tool recommended OAC the least often (14.91%). OAC treatment recommendations varied considerably when stroke risk was moderate or high (CHA₂DS₂-VASc > 0). Actual OAC use/non-use was highly discordant (>40%) with all of the guidelines or decision tools reflecting substantial opportunities to improve AF OAC decisions.
已发布的心房颤动(AF)指南和决策工具提供了口服抗凝药(OAC)的推荐建议;然而,它们对中风和出血风险的考量有所不同。我们研究的目的是:(i)比较2012年美国胸科医师学会指南、2012年欧洲心脏病学会(ESC)指南、2014年美国心脏协会(AHA)指南以及Casciano和LaHaye发布的两个决策工具在OAC推荐建议方面的差异;(ii)比较在整个研究人群以及按中风/出血风险分层的人群中,这些推荐建议与实际OAC使用情况的一致性。一项使用2001 - 2013年Lifelink理赔数据的横断面研究被用于对比这些决策辅助工具的治疗推荐建议。采用CHA₂DS₂ - VASc和HAS - BLED算法将15129例AF患者分为九个中风/出血风险组,以研究治疗推荐建议的差异以及与实际OAC使用/未使用情况的一致性。当CHA₂DS₂ - VASc = 1时设定推荐使用OAC的AHA指南推荐OAC的频率最高(86.30%),而LaHaye工具推荐OAC的频率最低(14.91%)。当中风风险为中度或高度(CHA₂DS₂ - VASc > 0)时,OAC治疗推荐建议差异很大。实际OAC的使用/未使用情况与所有指南或决策工具的一致性都很低(>40%),这表明在改善AF的OAC决策方面有很大的机会。