Ritchey Matthew, Tsipas Stavros, Loustalot Fleetwood, Wozniak Gregory
Division for Heart Disease and Stroke Prevention, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia, United States of America.
Health Outcomes Group, American Medical Association, Chicago, Illinois, United States of America.
PLoS One. 2016 Jul 18;11(7):e0159366. doi: 10.1371/journal.pone.0159366. eCollection 2016.
Effective hypertension management often necessitates patients' adherence to the blood pressure (BP)-lowering medication regimen they are prescribed. Patients' adherence to that regimen can be affected by prescription- and payment-related factors that are typically controlled by prescribers, filling pharmacies, pharmacy benefit managers, and/or patients' health insurance plans. This study describes patterns and changes from 2009 to 2014 in factors that the literature reports are associated with increased adherence to BP-lowering medication.
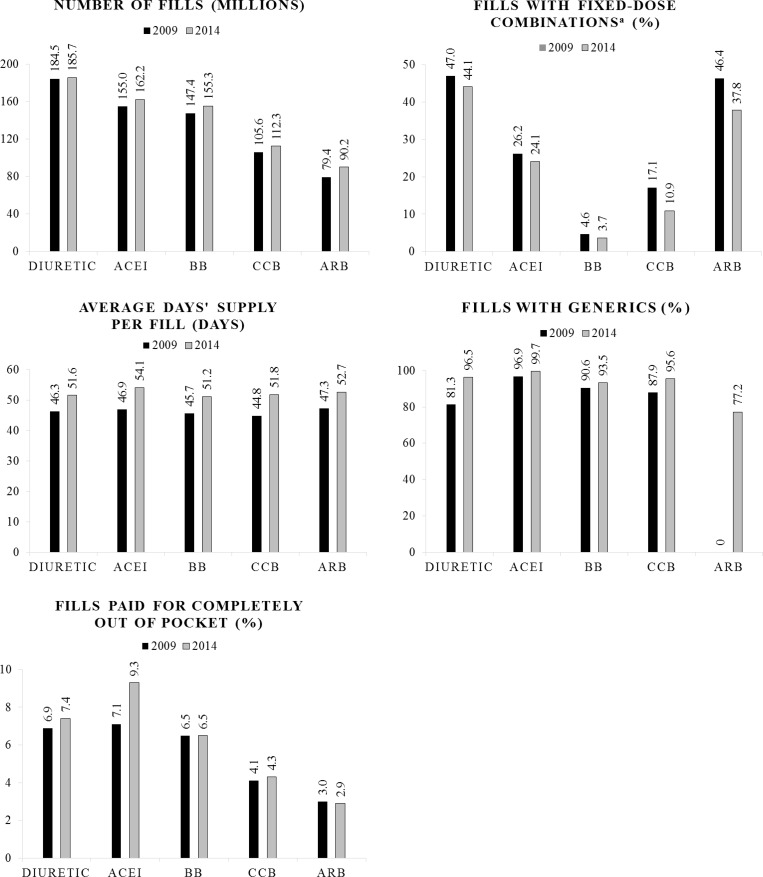
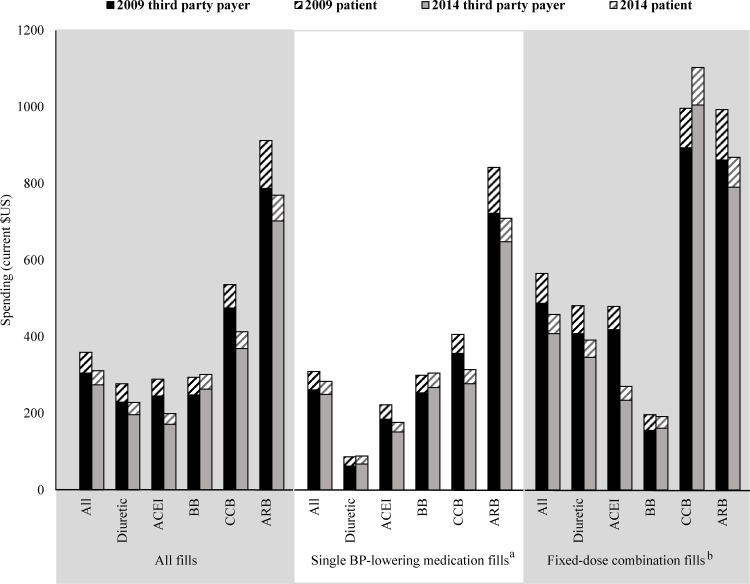
We use a robust source of United States prescription sales data-IMS Health's National Prescription Audit-to describe BP-lowering medication fill counts and spending in 2009 compared with 2014. Moreover, we describe patterns and changes in adherence-promoting factors across age groups, payment sources, and medication classes. From 2009 to 2014, the BP-lowering medication prescription fill count increased from 613.7 million to 653.0 million. Encouraging changes in adherence-promoting factors included: the share of generic fills increased from 82.5% to 95.0%; average days' supply per fill increased from 45.9 to 51.8 days; and average total (patient contribution) spending per years' supply decreased from $359 ($54) to $311 ($37). Possibly undesirable changes included: the percentage of fills for fixed-dose combinations decreased from 17.1% to 14.2% and acquired via mail order decreased from 10.7% to 8.2%. In 2014: 653.0 million fills occurred accounting for $28.81B in spending; adults aged 45-64 years had the highest percentage of fixed-dose combinations fills (16.9%); and fills with Medicaid as the payment source had the lowest average patient spending per fill ($1.19).
We identified both encouraging and possibly undesirable patterns and changes from 2009 to 2014 in factors that promote adherence to BP-lowering medications during this period. Continued tracking of these metrics using pharmacy sales data can help identify areas that can be addressed by clinical and policy interventions to improve adherence for medications commonly used to treat hypertension.
有效的高血压管理通常需要患者坚持服用所开具的降压药物治疗方案。患者对该方案的依从性可能会受到与处方和支付相关的因素影响,这些因素通常由开处方者、配药药房、药品福利管理机构和/或患者的健康保险计划控制。本研究描述了2009年至2014年期间文献报道的与降压药物依从性增加相关的因素的模式和变化。
我们使用美国处方销售数据的可靠来源——艾美仕市场研究公司的全国处方审计,来描述2009年与2014年相比的降压药物配药计数和支出情况。此外,我们描述了不同年龄组、支付来源和药物类别中促进依从性因素的模式和变化。从2009年到2014年,降压药物的处方配药计数从6.137亿增加到6.53亿。促进依从性因素的积极变化包括:通用名药物配药的比例从82.5%增加到95.0%;每次配药的平均供应天数从45.9天增加到51.8天;每年供应的平均总(患者自付)支出从359美元(54美元)降至311美元(37美元)。可能不理想的变化包括:固定剂量组合药物的配药比例从17.1%降至14.2%,通过邮购获得的比例从10.7%降至8.2%。2014年:发生了6.53亿次配药,支出达288.1亿美元;45至64岁的成年人固定剂量组合药物的配药比例最高(16.9%);以医疗补助作为支付来源的配药每次的平均患者支出最低(1.19美元)。
我们确定了2009年至2014年期间在促进降压药物依从性的因素方面既有令人鼓舞的模式和变化,也有可能不理想的情况。利用药房销售数据持续跟踪这些指标有助于确定临床和政策干预可以解决的领域,以提高常用于治疗高血压药物的依从性。