Department of Neurological Surgery, University of California, San Francisco, San Francisco, California, United States.
Departments of Neurological Surgery and Epidemiology and Biostatistics, University of California, San Francisco, California, United States.
Global Spine J. 2016 Aug;6(5):452-8. doi: 10.1055/s-0035-1565258. Epub 2015 Oct 25.
Retrospective review.
Intraoperative motor evoked potential (MEP) monitoring in spine surgery may assist surgeons in taking corrective measures to prevent neurologic deficits. The efficacy of monitoring MEPs intraoperatively in patients with myelopathy from nondegenerative causes has not been quantified. We compared the sensitivity and specificity of intraoperative MEP monitoring in patients with myelopathy caused by nondegenerative processes to patients with degenerative cervicothoracic spondylotic myelopathy (CSM).
We retrospectively reviewed our myelopathy surgical cases during a 1-year period to identify patients with degenerative CSM and CSM of nondegenerative causes and collected data on intraoperative MEP changes and postoperative new deficits. Categorical variables were analyzed by Fisher exact test. Receiver operator curves assessed intraoperative MEP monitoring performance in the two groups.
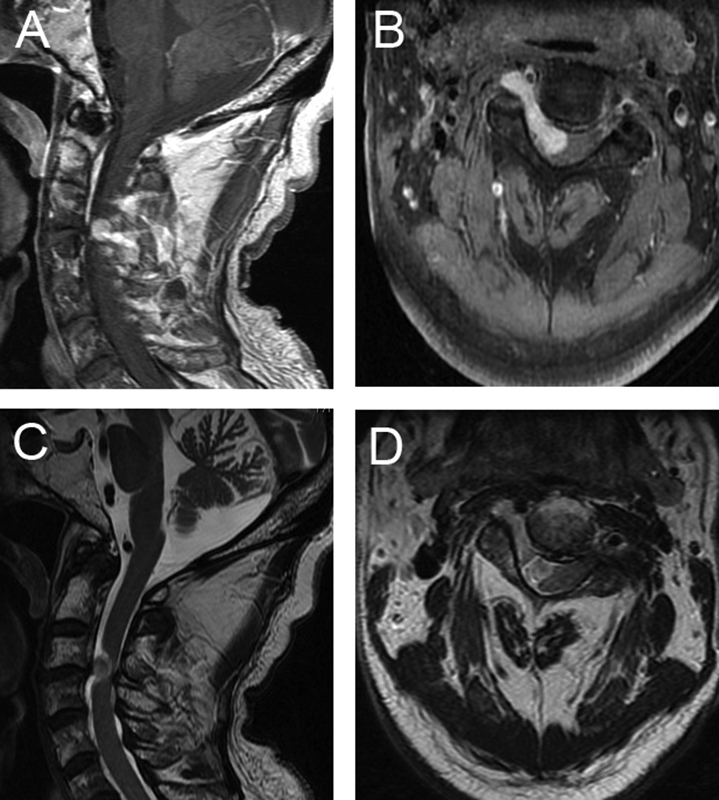
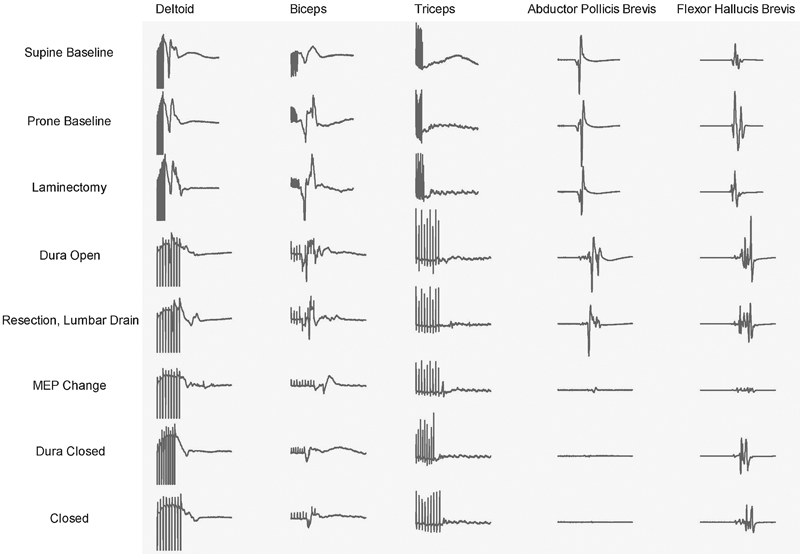
In all, 144 patients were identified: 102 had degenerative CSM and 42 had CSM of nondegenerative causes (24 extra-axial tumors, 12 infectious processes, 5 traumatic fractures, and 1 rheumatoid arthritis). For degenerative CSM, there were 11 intraoperative MEP alerts and 7 new deficits (p < 0.001). The corresponding sensitivity was 71% and the specificity was 94%. In the nondegenerative group, there were 11 intraoperative MEP alerts and 3 deficits, which was not significant (p > 0.99). The sensitivity (33%) and specificity (74%) were lower. Among patients with degenerative CSM, the model performed well for predicting postoperative deficits (area under the curve [AUC] 0.826), which appeared better than the nondegenerative group, although it did not reach statistical significance (AUC 0.538, p = 0.16).
Based on this large retrospective analysis, intraoperative MEP monitoring in surgery for nondegenerative CSM cases appears to be less sensitive to cord injury and less predictive of postoperative deficits when compared with degenerative CSM cases.
回顾性研究。
脊柱手术中术中运动诱发电位(MEP)监测可以帮助外科医生采取纠正措施,以防止神经功能缺损。非退行性病因引起的脊髓病患者术中监测 MEP 的效果尚未量化。我们比较了非退行性病变引起的脊髓病患者与退行性颈胸段脊髓病(CSM)患者术中 MEP 监测的敏感性和特异性。
我们回顾性分析了 1 年内脊髓病手术病例,以确定退行性 CSM 和非退行性 CSM 患者,并收集术中 MEP 变化和术后新出现的神经功能缺损数据。采用 Fisher 确切检验分析分类变量。受试者工作特征曲线评估了两组患者术中 MEP 监测的性能。
共确定 144 例患者:102 例为退行性 CSM,42 例为非退行性 CSM(24 例为轴外肿瘤,12 例为感染性疾病,5 例为外伤性骨折,1 例为类风湿关节炎)。对于退行性 CSM,有 11 次术中 MEP 警报和 7 次新出现的神经功能缺损(p<0.001)。相应的敏感性为 71%,特异性为 94%。在非退行性组中,有 11 次术中 MEP 警报和 3 次神经功能缺损,但无显著差异(p>0.99)。敏感性(33%)和特异性(74%)较低。在退行性 CSM 患者中,该模型对预测术后神经功能缺损的效果良好(曲线下面积[AUC]为 0.826),这似乎优于非退行性组,尽管差异无统计学意义(AUC 为 0.538,p=0.16)。
基于这项大型回顾性分析,与退行性 CSM 病例相比,非退行性 CSM 病例术中 MEP 监测对脊髓损伤的敏感性似乎较低,对术后神经功能缺损的预测性也较低。