Division of Cardiovascular Diseases, Department of Medicine, University of Mississippi Medical Center, Jackson.
Department of Medicine, Jackson Heart Study, University of Mississippi Medical Center, Jackson.
JAMA Cardiol. 2016 Apr 1;1(1):15-25. doi: 10.1001/jamacardio.2015.0300.
Cardiovascular risk assessment is a fundamental component of prevention of cardiovascular disease (CVD). However, commonly used prediction models have been formulated in primarily or exclusively white populations. Whether risk assessment in black adults is dissimilar to that in white adults is uncertain.
To develop and validate risk prediction models for CVD incidence in black adults, incorporating standard risk factors, biomarkers, and subclinical disease.
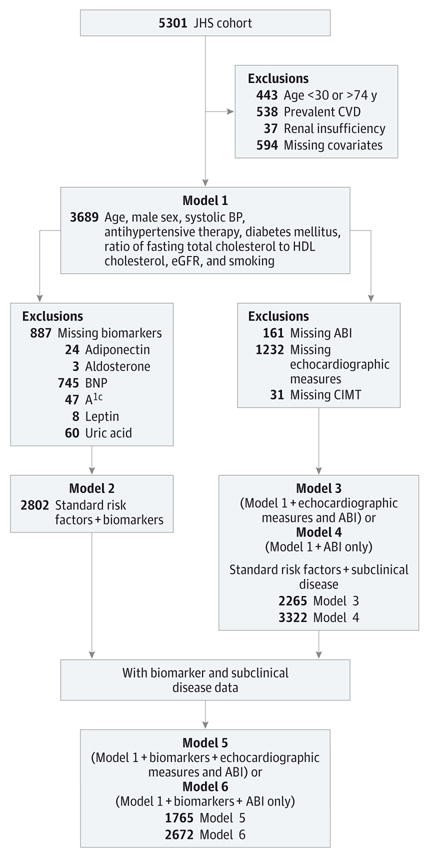
DESIGN, SETTING, AND PARTICIPANTS: The Jackson Heart Study (JHS), a longitudinal community-based study of 5301 black adults in Jackson, Mississippi. Inclusive study dates were the date of a participant's first visit (September 2000 to March 2004) to December 31, 2011. The median (75th percentile) follow-up was 9.1 (9.7) years. The dates of the analysis were August 2013 to May 2015. Measurements included standard risk factors, including age, sex, body mass index, systolic and diastolic blood pressure, ratio of fasting total cholesterol to high-density lipoprotein cholesterol, estimated glomerular filtration rate, antihypertensive therapy, diabetes mellitus, and smoking; blood biomarkers; and subclinical disease measures, including ankle-brachial index, carotid intimal-medial thickness, and echocardiographic left ventricular hypertrophy and systolic dysfunction.
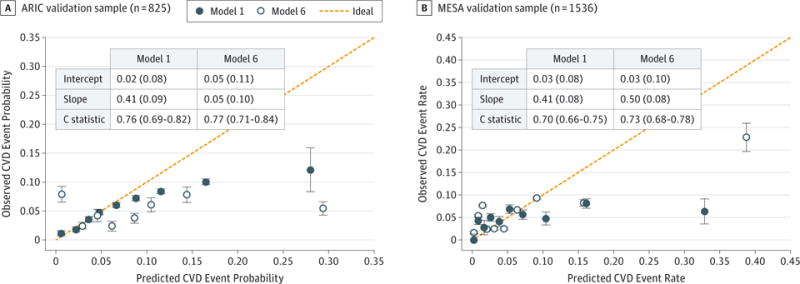
Incident CVD event was defined as the first occurrence of myocardial infarction, coronary heart disease death, congestive heart failure, stroke, incident angina, or intermittent claudication. Model performance was compared with the American College of Cardiology/American Heart Association (ACC/AHA) CVD risk algorithm and the Framingham Risk Score (FHS) refitted to the JHS data and evaluated in the Atherosclerosis Risk in Communities (ARIC) and Multi-Ethnic Study of Atherosclerosis cohorts.
The study cohort comprised 3689 participants with mean (SD) age at baseline was 53 (11) years, and 64.8% (n = 2390) were female. Over a median of 9.1 years, 270 participants (166 women) experienced a first CVD event. A simple combination of standard CVD risk factors, B-type natriuretic peptide, and ankle-brachial index (model 6) yielded modest improvement over a model without B-type natriuretic peptide and ankle-brachial index (C statistic, 0.79; 95% CI, 0.75-0.83 [relative integrated discrimination improvement, 0.22; 95% CI, 0.15-0.30]). However, the reclassification improvement was not substantially different between model 6 and the ACC/AHA CVD Pooled Cohort risk equations or between model 6 and the FHS. The models discriminated reasonably well in the ARIC and Multi-Ethnic Study of Atherosclerosis data (C statistic range, 0.70-0.77).
Our findings using the JHS data in the present study are valuable because they confirm that current FHS and ACC/AHA risk algorithms work well in black individuals and are not easily improved on. A unique risk calculator for black adults may not be necessary.
心血管风险评估是预防心血管疾病(CVD)的基本组成部分。然而,常用的预测模型主要或完全是在白种人群中制定的。黑种成年人的风险评估是否与白种成年人不同尚不确定。
制定并验证黑种成年人 CVD 发病风险预测模型,纳入标准风险因素、生物标志物和亚临床疾病。
设计、地点和参与者:Jackson 心脏研究(JHS)是一项在密西西比州 Jackson 市的 5301 名黑种成年人中进行的纵向社区基础研究。纳入研究的日期为参与者首次就诊的日期(2000 年 9 月至 2004 年 3 月)至 2011 年 12 月 31 日。中位数(75 百分位数)随访时间为 9.1(9.7)年。分析日期为 2013 年 8 月至 2015 年 5 月。测量包括标准风险因素,包括年龄、性别、体重指数、收缩压和舒张压、空腹总胆固醇与高密度脂蛋白胆固醇的比值、估计肾小球滤过率、降压治疗、糖尿病和吸烟;血液生物标志物;以及亚临床疾病指标,包括踝臂指数、颈动脉内膜中层厚度和超声心动图左心室肥厚和收缩功能障碍。
首发 CVD 事件定义为心肌梗死、冠心病死亡、充血性心力衰竭、卒中等首次发生、心绞痛或间歇性跛行。与美国心脏病学会/美国心脏协会(ACC/AHA)CVD 风险算法和重新拟合 JHS 数据的 Framingham 风险评分(FHS)进行比较,并在 Atherosclerosis Risk in Communities(ARIC)和 Multi-Ethnic Study of Atherosclerosis 队列中进行评估。
研究队列包括 3689 名参与者,基线时的平均(SD)年龄为 53(11)岁,64.8%(n=2390)为女性。在中位数为 9.1 年的随访期间,270 名参与者(166 名女性)经历了首发 CVD 事件。标准 CVD 风险因素、B 型利钠肽和踝臂指数的简单组合(模型 6)在没有 B 型利钠肽和踝臂指数的模型的基础上略有改善(C 统计量,0.79;95%CI,0.75-0.83[相对综合判别改善,0.22;95%CI,0.15-0.30])。然而,模型 6 与 ACC/AHA CVD Pooled Cohort 风险方程或模型 6 与 FHS 之间的重新分类改善并没有显著差异。模型在 ARIC 和 Multi-Ethnic Study of Atherosclerosis 数据中具有较好的区分度(C 统计量范围,0.70-0.77)。
本研究使用 JHS 数据的发现是有价值的,因为它们证实了目前的 FHS 和 ACC/AHA 风险算法在黑种人群中效果良好,且不易改进。为黑种成年人制定独特的风险计算器可能不是必需的。