van der Plas Willemijn Y, Engelsman Anton F, Özyilmaz Akin, van der Horst-Schrivers Anouk N, Meijer Kornelis, van Dam Gooitzen M, Pol Robert A, de Borst Martin H, Kruijff Schelto
Department of Surgery, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Department of Surgery, Academic Medical Center, Amsterdam, The Netherlands.
Ann Surg Oncol. 2017 Jan;24(1):15-22. doi: 10.1245/s10434-016-5450-6. Epub 2016 Jul 26.
Hyperparathyroidism (HPT), both secondary and tertiary, is common in patients with end-stage renal disease, and is associated with severe bone disorders, cardiovascular complications, and increased mortality. Since the introduction of calcimimetics in 2004, treatment of HPT has shifted from surgery to predominantly medical therapy.
The aim of this study was to evaluate the impact of this change of management on the HPT patient population before undergoing (sub-)total parathyroidectomy (PTx).
Overall, 119 patients with secondary or tertiary HPT undergoing PTx were included in a retrospective, single-center cohort. Group A, who underwent PTx before January 2005, was compared with group B, who underwent PTx after January 2005. Patient characteristics, time interval between HPT diagnosis and PTx, and postoperative complications were compared.
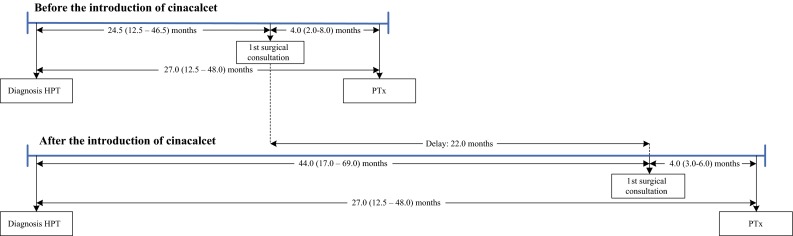
Group A comprised 70 (58.8 %) patients and group B comprised 49 (41.2 %) patients. The median interval between HPT diagnosis and PTx was 27 (interquartile range [IQR] 12.5-48.0) and 49 (IQR 21.0-75.0) months for group A and B, respectively (p = 0.007). Baseline characteristics were similar among both groups. The median preoperative serum parathyroid hormone (PTH) level was 936 pg/mL (IQR 600-1273) for group A versus 1091 pg/mL (IQR 482-1373) for group B (p = 0.38). PTx resulted in a dramatic PTH reduction (less than twofold the upper limit: A, 80.0 %; B, 85.4 %), and postoperative complication rates were low in both groups (A: 7.8 %; B: 10.2 %) [p = 0.66].
The introduction of calcimimetics in 2004 is associated with a significant 2-year delay of surgery with continuously elevated preoperative PTH levels, while parathyroid surgery, even in a fragile population, is considered a safe and effective procedure.
继发性和三发性甲状旁腺功能亢进(HPT)在终末期肾病患者中很常见,并且与严重的骨骼疾病、心血管并发症及死亡率增加相关。自2004年拟钙剂问世以来,HPT的治疗已从手术为主转变为主要采用药物治疗。
本研究旨在评估这种治疗方式的改变对接受(次)全甲状旁腺切除术(PTx)之前的HPT患者群体的影响。
总体而言,119例接受PTx的继发性或三发性HPT患者被纳入一项回顾性单中心队列研究。将2005年1月之前接受PTx的A组与2005年1月之后接受PTx的B组进行比较。比较患者特征、HPT诊断与PTx之间的时间间隔以及术后并发症。
A组有70例(58.8%)患者,B组有49例(41.2%)患者。A组和B组HPT诊断与PTx之间的中位间隔分别为27个月(四分位间距[IQR]12.5 - 48.0)和49个月(IQR 21.0 - 75.0)(p = 0.007)。两组的基线特征相似。A组术前血清甲状旁腺激素(PTH)水平的中位数为936 pg/mL(IQR 600 - 1273),而B组为1091 pg/mL(IQR 482 - 1373)(p = 0.38)。PTx导致PTH显著降低(低于上限的两倍:A组为80.0%;B组为85.4%),且两组术后并发症发生率均较低(A组:7.8%;B组:10.2%)[p = 0.66]。
2004年拟钙剂的引入与手术延迟2年且术前PTH水平持续升高显著相关,而甲状旁腺手术即使在脆弱人群中也是一种安全有效的手术。