Ritte Rebecca, Luke Joanne, Nelson Craig, Brown Alex, O'Dea Kerin, Jenkins Alicia, Best James D, McDermott Robyn, Daniel Mark, Rowley Kevin
Onemda Group, Indigenous Health Equity Unit, Centre for Health Equity, Melbourne School of Population and Global Health, The University of Melbourne, VIC, Melbourne, 3010, Australia.
Western Health, Footscray, VIC, 3011, Australia.
BMC Nephrol. 2016 Aug 5;17(1):113. doi: 10.1186/s12882-016-0328-1.
Chronic kidney disease (CKD) and end-stage-kidney disease (ESKD) continue to be under-diagnosed and a major burden for Aboriginal communities in central Australia. The aim of this study was to examine the risk of poor clinical outcomes associated with elevated albumin-to-creatinine ratio (ACR) among Aboriginal people in central Australia.
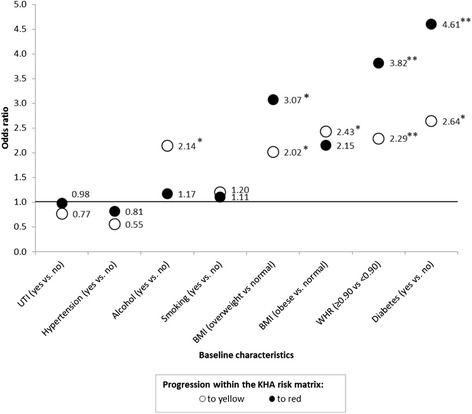
Cox proportional hazards models were used to estimate the risk of end stage kidney disease (ESKD), dialysis, CVD (cardiovascular disease) and mortality associated with participants' baseline albuminuria reading from a 10-year cohort study of Aboriginal people (n = 623) from three communities in central Australia. Predictors of progression of albuminuria were also examined in the context of the Kidney Health Australia (KHA) Risk Matrix.
A baseline ACR level of ≥3.5 mg/mmol was associated with an almost 10-fold increased risk of ESKD (95%CI 2.07-43.8) and a 15-fold risk of dialysis (95%CI 1.89-121). Albuminuria ≥3.5 mg/mmol was also associated with a borderline 63 % increased risk of CVD (95%CI 0.98-2.71). No significant association was observed with mortality from all-causes or chronic disease. Diabetes and a waist-to-hip ratio ≥0.90 independently predicted a two-fold increased risk of a progression to higher ACR levels.
A single measure of moderately increased albuminuria was a strong predictor of renal failure in this population. A single spot urine ACR analysis in conjunction with the KHA Risk Matrix may be a useful and efficient strategy to screen for risk of CKD and progression to dialysis in remote communities. A focus on individuals with diabetes and/or central obesity for strategies to avoid increases in albuminuria may also prevent future CKD and CVD complications.
慢性肾脏病(CKD)和终末期肾病(ESKD)在澳大利亚中部原住民社区的诊断率仍然较低,且是一个主要负担。本研究的目的是调查澳大利亚中部原住民中与白蛋白与肌酐比值(ACR)升高相关的不良临床结局风险。
采用Cox比例风险模型,根据澳大利亚中部三个社区的10年原住民队列研究(n = 623)中参与者的基线蛋白尿读数,估计终末期肾病(ESKD)、透析、心血管疾病(CVD)和死亡风险。还在澳大利亚肾脏健康(KHA)风险矩阵的背景下研究了蛋白尿进展的预测因素。
基线ACR水平≥3.5mg/mmol与ESKD风险增加近10倍(95%CI 2.07 - 43.8)和透析风险增加15倍(95%CI 1.89 - 121)相关。蛋白尿≥3.5mg/mmol也与CVD风险增加63%(95%CI 0.98 - 2.71)接近相关。未观察到与全因或慢性病死亡的显著关联。糖尿病和腰臀比≥0.90独立预测ACR水平升高的风险增加两倍。
在该人群中,单次测量中度蛋白尿增加是肾衰竭的有力预测指标。结合KHA风险矩阵进行单次随机尿ACR分析可能是筛查偏远社区CKD风险和进展至透析的有用且有效的策略。关注患有糖尿病和/或中心性肥胖的个体以避免蛋白尿增加的策略,也可能预防未来的CKD和CVD并发症。