Oh Woo Jin, Chung Arthur Minwoo, Kim Jee Soon, Han Ji Heun, Hong Sung Hoo, Lee Ji Yeol, Choi Yeong Jin
Department of Hospital Pathology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Department of Urology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
J Pathol Transl Med. 2016 Sep;50(5):345-54. doi: 10.4132/jptm.2016.06.14. Epub 2016 Aug 7.
The pathologic distinction between high-grade prostate adenocarcinoma (PAC) involving the urinary bladder and high-grade urothelial carcinoma (UC) infiltrating the prostate can be difficult. However, making this distinction is clinically important because of the different treatment modalities for these two entities.
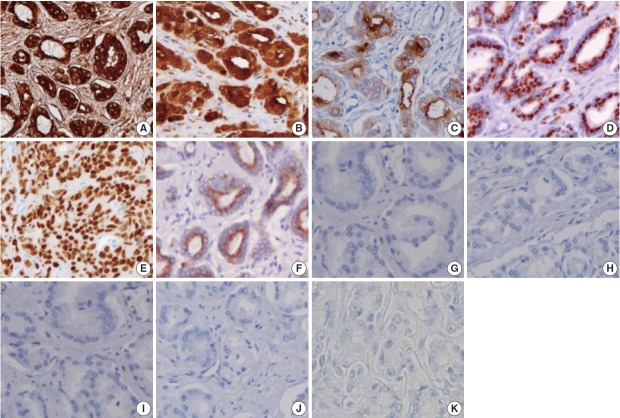
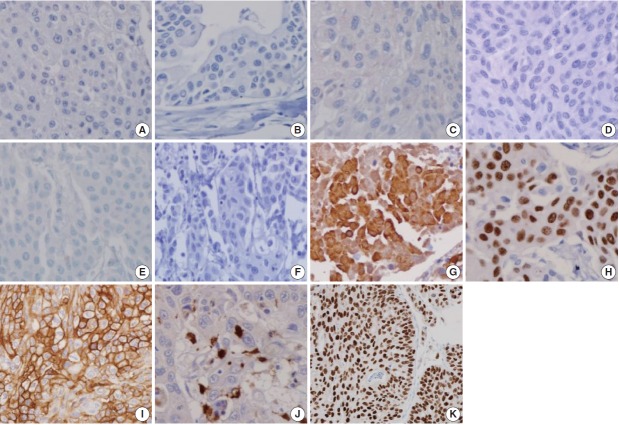
A total of 249 patient cases (PAC, 111 cases; UC, 138 cases) collected between June 1995 and July 2009 at Seoul St. Mary's Hospital were studied. An immunohistochemical evaluation of prostatic markers (prostate-specific antigen [PSA], prostate-specific membrane antigen [PSMA], prostate acid phosphatase [PAP], P501s, NKX3.1, and α-methylacyl coenzyme A racemase [AMACR]) and urothelial markers (CK34βE12, p63, thrombomodulin, S100P, and GATA binding protein 3 [GATA3]) was performed using tissue microarrays from each tumor.
The sensitivities of prostatic markers in PAC were 100% for PSA, 83.8% for PSMA, 91.9% for PAP, 93.7% for P501s, 88.3% for NKX 3.1, and 66.7% for AMACR. However, the urothelial markers CK34βE12, p63, thrombomodulin, S100P, and GATA3 were also positive in 1.8%, 0%, 0%, 3.6%, and 0% of PAC, respectively. The sensitivities of urothelial markers in UC were 75.4% for CK34βE12, 73.9% for p63, 45.7% for thrombomodulin, 22.5% for S100P, and 84.8% for GATA3. Conversely, the prostatic markers PSA, PSMA, PAP, P501s, NKX3.1, and AMACR were also positive in 9.4%, 0.7%, 18.8%, 0.7%, 0%, and 8.7% of UCs, respectively.
Prostatic and urothelial markers, including PSA, NKX3.1, p63, thrombomodulin, and GATA3 are very useful for differentiating PAC from UC. The optimal combination of prostatic and urothelial markers could improve the ability to differentiate PAC from UC pathologically.
区分累及膀胱的高级别前列腺腺癌(PAC)和浸润前列腺的高级别尿路上皮癌(UC)在病理上可能存在困难。然而,由于这两种实体的治疗方式不同,做出这种区分在临床上具有重要意义。
对1995年6月至2009年7月在首尔圣玛丽医院收集的249例患者病例(PAC,111例;UC,138例)进行研究。使用来自每个肿瘤的组织微阵列对前列腺标志物(前列腺特异性抗原[PSA]、前列腺特异性膜抗原[PSMA]、前列腺酸性磷酸酶[PAP]、P501s、NKX3.1和α-甲基酰基辅酶A消旋酶[AMACR])和尿路上皮标志物(CK34βE12、p63、血栓调节蛋白、S100P和GATA结合蛋白3[GATA3])进行免疫组织化学评估。
PAC中前列腺标志物的敏感性分别为:PSA为100%,PSMA为83.8%,PAP为91.9%,P501s为93.7%,NKX3.1为88.3%,AMACR为66.7%。然而,尿路上皮标志物CK34βE12、p63、血栓调节蛋白、S100P和GATA3在PAC中分别有1.8%、0%、0%、3.6%和0%呈阳性。UC中尿路上皮标志物的敏感性分别为:CK34βE12为75.4%,p63为73.9%,血栓调节蛋白为45.7%,S100P为22.5%,GATA3为84.8%。相反,前列腺标志物PSA、PSMA、PAP、P501s、NKX3.1和AMACR在UC中分别有9.4%、0.7%、18.8%、0.7%、0%和8.7%呈阳性。
包括PSA、NKX3.1、p63、血栓调节蛋白和GATA3在内的前列腺和尿路上皮标志物对于区分PAC和UC非常有用。前列腺和尿路上皮标志物的最佳组合可以提高病理上区分PAC和UC的能力。