Cozzi Gabriella D, Samuel Jacob M, Fromal Jason T, Keene Spencer, Crispens Marta A, Khabele Dineo, Beeghly-Fadiel Alicia
Division of Epidemiology, Department of Medicine, Vanderbilt University Medical Center, 2525 West End Avenue, 838-A, Nashville, TN, 37203, USA.
Division of Gynecologic Oncology, Department of Obstetics and Gynecology, Vanderbilt University Medical Center, Nashville, TN, 37203, USA.
BMC Cancer. 2016 Aug 8;16:612. doi: 10.1186/s12885-016-2660-z.
Thrombocytosis has been associated with poor ovarian cancer prognosis. However, comparisons of thresholds to define thrombocytosis and evaluation of relevant timing of platelet measurement has not been previously conducted.
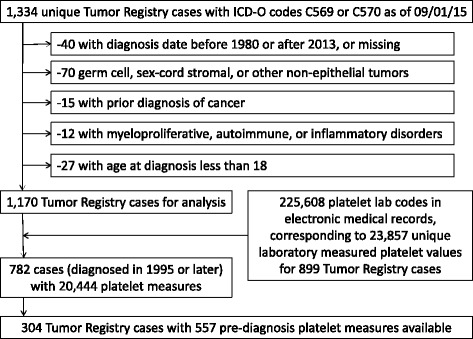
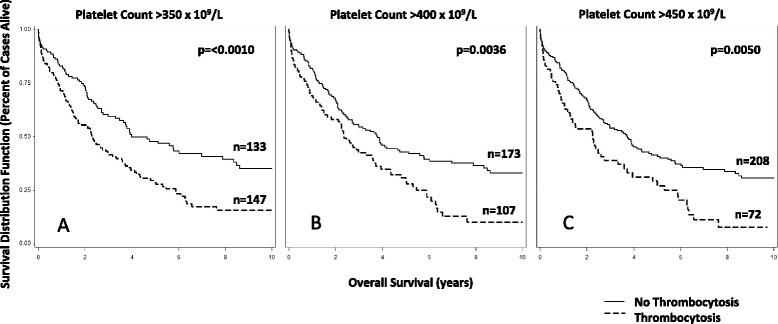
We selected Tumor Registry confirmed ovarian, primary peritoneal, and fallopian tube cancer cases diagnosed between 1995-2013 from the Vanderbilt University Medical Center. Laboratory measured platelet values from electronic medical records (EMR) were used to determine thrombocytosis at three thresholds: a platelet count greater than 350, 400, or 450 × 10(9)/liter. Timing was evaluated with 5 intervals: on the date of diagnosis, and up to 1, 2, 4, and 8 weeks prior to the date of diagnosis. Cox regression was used to calculate hazard ratios (HR) and confidence intervals (CI) for association with overall survival; adjustment included age, stage, grade, and histologic subtype of disease.
Pre-diagnosis platelet measures were available for 136, 241, 280, 297, and 304 cases in the five intervals. The prevalence of thrombocytosis decreased with increasing thresholds and was generally consistent across the five time intervals, ranging from 44.8-53.2 %, 31.6-39.4 %, and 19.9-26.1 % across the three thresholds. Associations with higher grade and stage of disease gained significance as the threshold increased. With the exception of the lowest threshold on the date of diagnosis (HR350: 1.55, 95 % CI: 0.97-2.47), all other survival associations were significant, with the highest reaching twice the risk of death for thrombocytosis on the date of diagnosis (HR400: 2.01, 95 % CI: 1.25-3.23).
Our EMR approach yielded associations comparable to published findings from medical record abstraction approaches. In addition, our results indicate that lower thrombocytosis thresholds and platelet measures up to 8 weeks before diagnosis may inform ovarian cancer characteristics and prognosis.
血小板增多症与卵巢癌预后不良相关。然而,此前尚未对定义血小板增多症的阈值以及血小板测量的相关时间点进行比较。
我们从范德比尔特大学医学中心选取了1995年至2013年间经肿瘤登记处确诊的卵巢癌、原发性腹膜癌和输卵管癌病例。利用电子病历(EMR)中实验室测量的血小板值,以三个阈值确定血小板增多症:血小板计数大于350、400或450×10⁹/升。时间点以5个时间段进行评估:诊断日期,以及诊断日期前1、2、4和8周。采用Cox回归计算与总生存期相关的风险比(HR)和置信区间(CI);调整因素包括疾病的年龄、分期、分级和组织学亚型。
在五个时间段中,分别有136、241、280、297和304例病例有诊断前血小板测量数据。血小板增多症的患病率随阈值升高而降低,且在五个时间段内总体一致,三个阈值下的患病率分别为44.8 - 53.2%、31.6 - 39.4%和19.9 - 26.1%。随着阈值升高,与疾病更高分级和分期的关联变得显著。除了诊断日期时最低阈值(HR350:1.55,95%CI:0.97 - 2.47)外,所有其他生存关联均显著,诊断日期时血小板增多症导致死亡风险最高可达两倍(HR400:2.01,95%CI:1.25 - 3.23)。
我们的EMR方法得出的关联与病历摘要方法发表的结果相当。此外,我们的结果表明,较低的血小板增多症阈值以及诊断前8周内的血小板测量可能有助于了解卵巢癌特征和预后。