Forte Brittany L, Slosky Lauren M, Zhang Hong, Arnold Moriah R, Staatz William D, Hay Meredith, Largent-Milnes Tally M, Vanderah Todd W
aDepartment of Pharmacology, College of Medicine, University of Arizona, Tucson, AZ, USA bDepartment of Physiology, Evelyn McKnight Brain Institute, College of Medicine, University of Arizona, Tucson, AZ, USA.
Pain. 2016 Dec;157(12):2709-2721. doi: 10.1097/j.pain.0000000000000690.
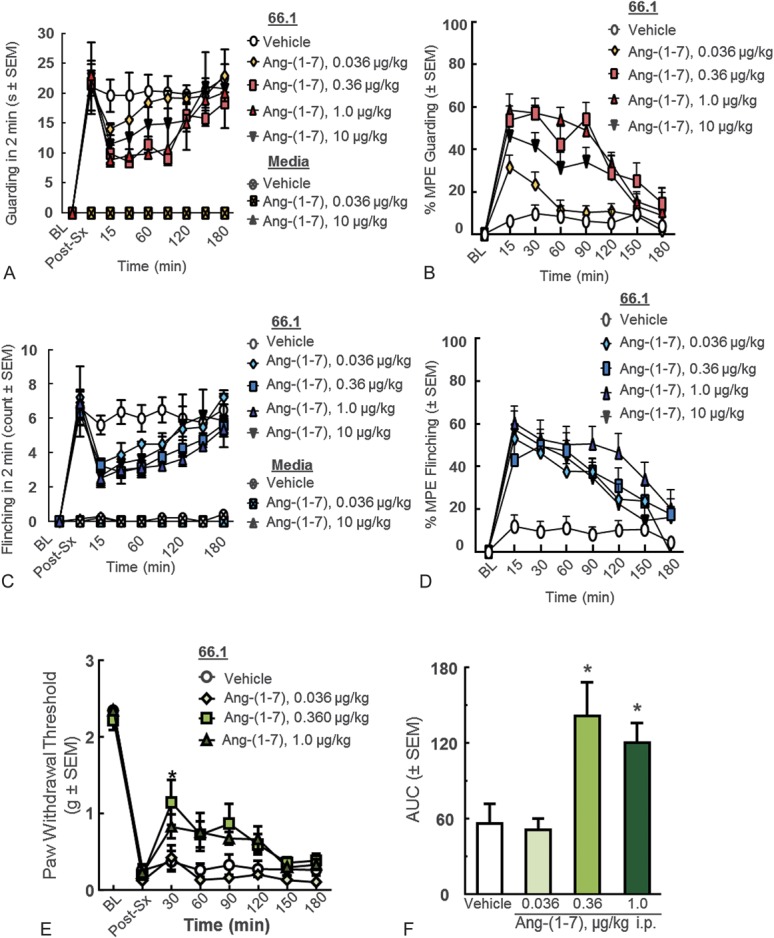
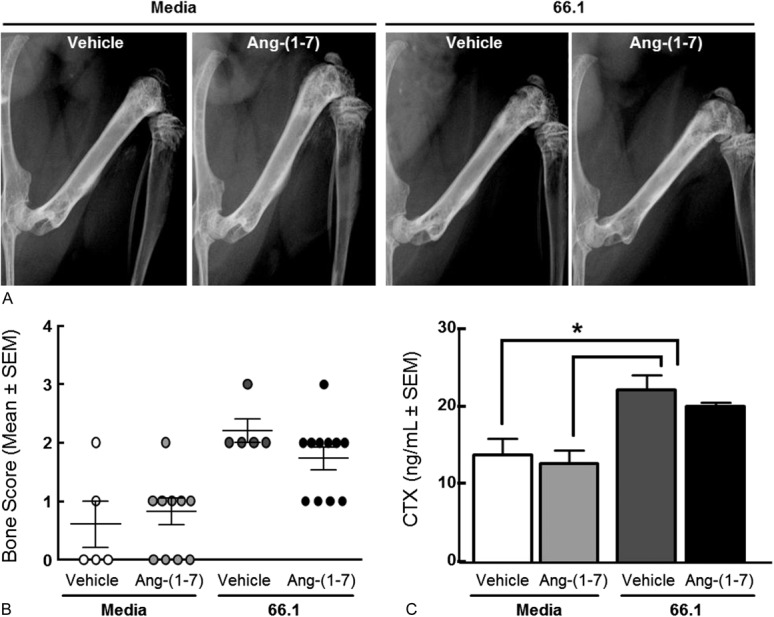
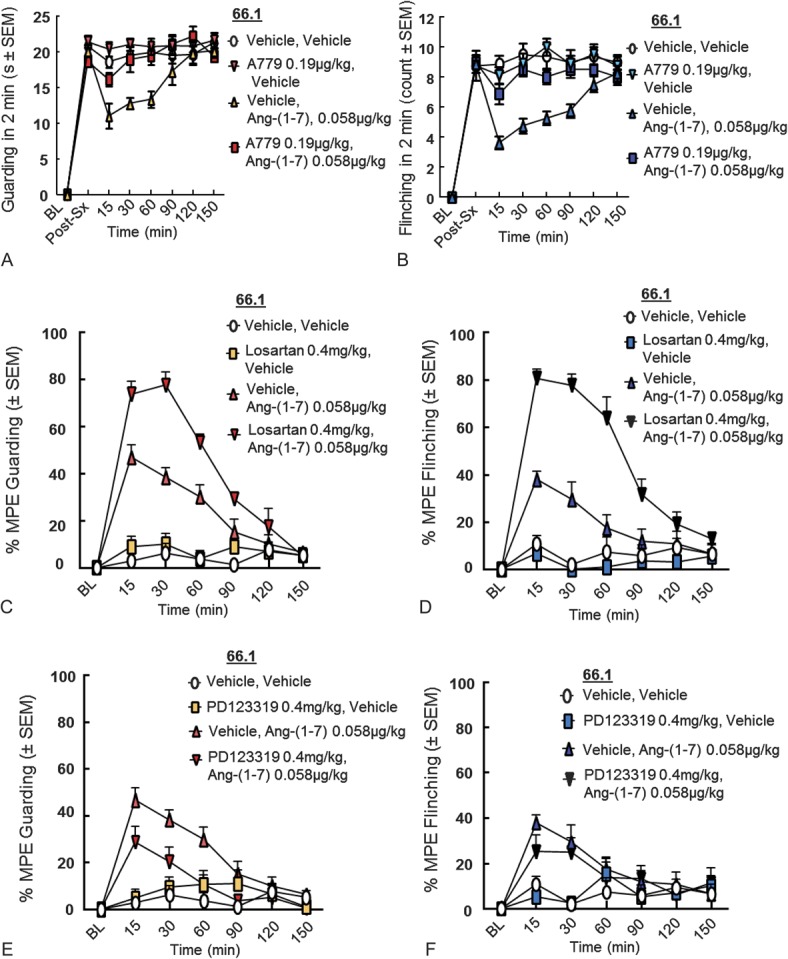
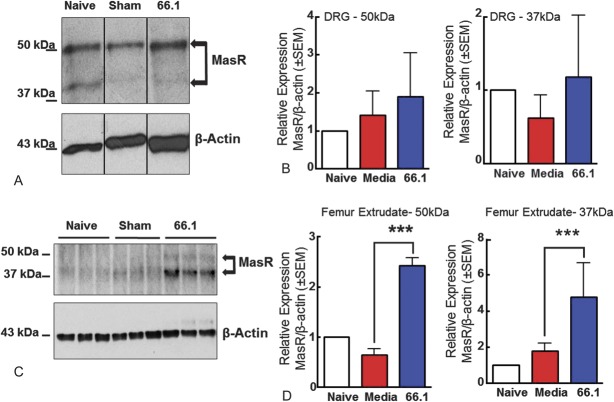
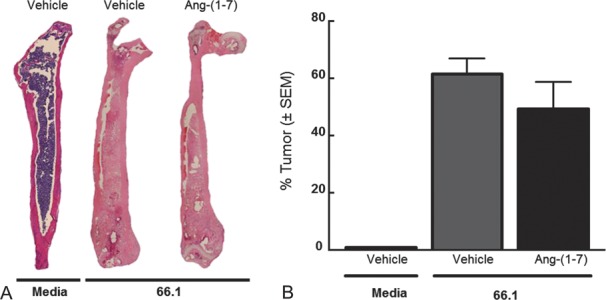
Many cancerous solid tumors metastasize to the bone and induce pain (cancer-induced bone pain [CIBP]). Cancer-induced bone pain is often severe because of enhanced inflammation, rapid bone degradation, and disease progression. Opioids are prescribed to manage this pain, but they may enhance bone loss and increase tumor proliferation, further compromising patient quality of life. Angiotensin-(1-7) (Ang-(1-7)) binds and activates the Mas receptor (MasR). Angiotensin-(1-7)/MasR activation modulates inflammatory signaling after acute tissue insult, yet no studies have investigated whether Ang-(1-7)/MasR play a role in CIBP. We hypothesized that Ang-(1-7) inhibits CIBP by targeting MasR in a murine model of breast CIBP. 66.1 breast cancer cells were implanted into the femur of BALB/cAnNHsd mice as a model of CIBP. Spontaneous and evoked pain behaviors were assessed before and after acute and chronic administration of Ang-(1-7). Tissues were collected from animals for ex vivo analyses of MasR expression, tumor burden, and bone integrity. Cancer inoculation increased spontaneous pain behaviors by day 7 that were significantly reduced after a single injection of Ang-(1-7) and after sustained administration. Preadministration of A-779 a selective MasR antagonist prevented this reduction, whereas pretreatment with the AT2 antagonist had no effect; an AT1 antagonist enhanced the antinociceptive activity of Ang-(1-7) in CIBP. Repeated Ang-(1-7) administration did not significantly change tumor burden or bone remodeling. Data here suggest that Ang-(1-7)/MasR activation significantly attenuates CIBP, while lacking many side effects seen with opioids. Thus, Ang-(1-7) may be an alternative therapeutic strategy for the nearly 90% of patients with advanced-stage cancer who experience excruciating pain.
许多癌性实体瘤会转移至骨骼并引发疼痛(癌性骨痛 [CIBP])。由于炎症加剧、骨快速降解和疾病进展,癌性骨痛往往较为严重。阿片类药物被用于治疗这种疼痛,但它们可能会加剧骨质流失并增加肿瘤增殖,进一步损害患者的生活质量。血管紧张素-(1-7)(Ang-(1-7))结合并激活Mas受体(MasR)。急性组织损伤后,血管紧张素-(1-7)/MasR激活可调节炎症信号传导,但尚无研究调查Ang-(1-7)/MasR在CIBP中是否起作用。我们假设在乳腺癌CIBP小鼠模型中,Ang-(1-7)通过靶向MasR抑制CIBP。将66.1乳腺癌细胞植入BALB/cAnNHsd小鼠的股骨中作为CIBP模型。在急性和慢性给予Ang-(1-7)之前和之后评估自发和诱发的疼痛行为。从动物身上收集组织用于MasR表达、肿瘤负荷和骨完整性的离体分析。接种癌症后第7天自发疼痛行为增加,单次注射Ang-(1-7)后以及持续给药后显著降低。预先给予选择性MasR拮抗剂A-779可阻止这种降低,而用AT2拮抗剂预处理则无效;AT1拮抗剂增强了Ang-(1-7)在CIBP中的镇痛活性。重复给予Ang-(1-7)并未显著改变肿瘤负荷或骨重塑。此处数据表明,Ang-(1-7)/MasR激活可显著减轻CIBP,同时缺乏阿片类药物所见的许多副作用。因此,对于近90%经历剧痛的晚期癌症患者,Ang-(1-7)可能是一种替代治疗策略。