Salomoni Sauro, Tucker Kylie, Hug François, McPhee Megan, Hodges Paul
The University of Queensland, Centre for Clinical Research Excellence in Spinal Pain, Injury and Health, School of Health and Rehabilitation Sciences, Brisbane, Australia.
The University of Queensland, School of Biomedical Sciences, Brisbane, Australia.
PLoS One. 2016 Aug 25;11(8):e0161487. doi: 10.1371/journal.pone.0161487. eCollection 2016.
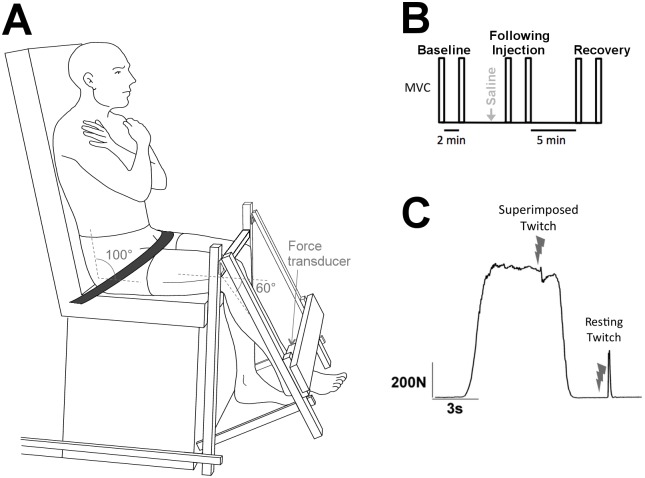
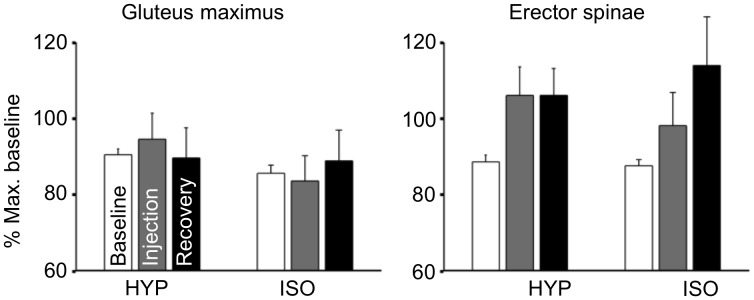
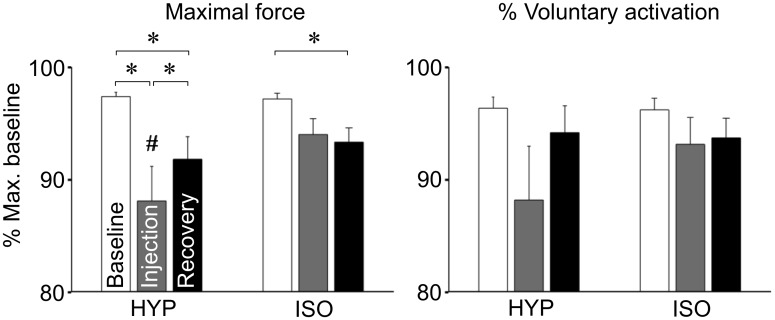
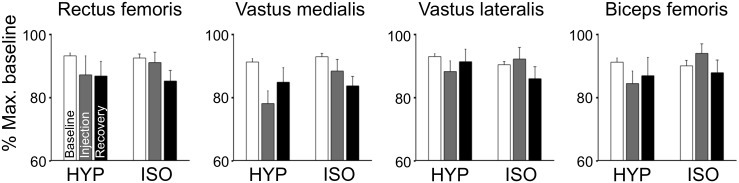
Although maximal voluntary contraction (MVC) force is reduced during pain, studies using interpolated twitch show no consistent reduction of voluntary muscle drive. The present study aimed to test if the reduction in MVC force during acute experimental pain could be explained by increased activation of antagonist muscles, weak voluntary activation at baseline, or changes in force direction. Twenty-two healthy volunteers performed maximal voluntary isometric knee extensions before, during, and after the effects of hypertonic (pain) and isotonic (control) saline injections into the infrapatellar fat pad. The MVC force, voluntary activation, electromyographic (EMG) activity of agonist, antagonist, and auxiliary (hip) muscles, and pain cognition and anxiety scores were recorded. MVC force was 9.3% lower during pain than baseline (p < 0.001), but there was no systematic change in voluntary activation. Reduced MVC force during pain was variable between participants (SD: 14%), and was correlated with reduced voluntary activation (r = 0.90), baseline voluntary activation (r = - 0.62), and reduced EMG amplitude of agonist and antagonist muscles (all r > 0.52), but not with changes in force direction, pain or anxiety scores. Hence, reduced MVC force during acute pain was mainly explained by deficits in maximal voluntary drive.
尽管在疼痛期间最大自主收缩(MVC)力会降低,但使用内插单收缩的研究表明,自主肌肉驱动并没有持续降低。本研究旨在测试急性实验性疼痛期间MVC力的降低是否可以通过拮抗肌激活增加、基线时自主激活较弱或力的方向变化来解释。22名健康志愿者在向髌下脂肪垫注射高渗(疼痛)和等渗(对照)盐水的影响之前、期间和之后进行了最大自主等长膝关节伸展。记录了MVC力、自主激活、主动肌、拮抗肌和辅助(髋)肌的肌电图(EMG)活动,以及疼痛认知和焦虑评分。疼痛期间的MVC力比基线时低9.3%(p < 0.001),但自主激活没有系统性变化。疼痛期间MVC力的降低在参与者之间存在差异(标准差:14%),并且与自主激活降低(r = 0.90)、基线自主激活(r = - 0.62)以及主动肌和拮抗肌的EMG幅度降低(所有r > 0.52)相关,但与力的方向变化、疼痛或焦虑评分无关。因此,急性疼痛期间MVC力的降低主要是由最大自主驱动不足所解释的。