Boegemann Martin, Schlack Katrin, Fischer Ann-Kathrin, Gerß Joachim, Steinestel Julie, Semjonow Axel, Schrader Andres Jan, Krabbe Laura-Maria
Department of Urology, Muenster University Medical Center, Muenster, Germany.
Institute of Biostatistics and Clinical Research of the Westfalian Wilhelms-University Muenster, Schmeddingstraße 56, D-48149 Muenster, Germany.
PLoS One. 2016 Sep 1;11(9):e0161959. doi: 10.1371/journal.pone.0161959. eCollection 2016.
Even though the exact mechanism is largely unknown until now, statins are supposed to improve survival outcomes in various malignancies. For prostate cancer however, statins are known to compete with dehydroepiandrosterone (DHEAS) for the transport into the cytosol both using the cell by the Solute Carrier Transporter and thus diminish the cellular uptake of DHEAS as a precursor of androgens. Abiraterone inhibits CYP17A1 and thus effectively decreases the production of all relevant androgens including DHEAS. In this study we examined whether statins still affect survival outcome in patients with metastatic castration resistant prostate cancer (mCRPC) when treated with Abiraterone.
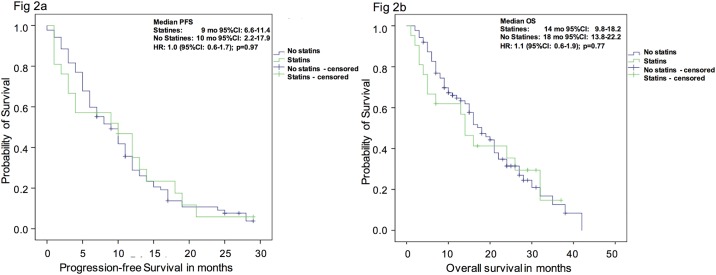
108 men with mCRPC treated with Abiraterone from 02/2010 to 07/2015 with (n = 21) or without (n = 87) concomitant treatment with statins were investigated. Progression free survival (PFS) and overall survival (OS) were analyzed using Kaplan-Meier-estimates and univariate Cox-regression analysis. The influence on best clinical benefit under Abiraterone treatment was analyzed with bivariate and multivariate logistic regression analysis.
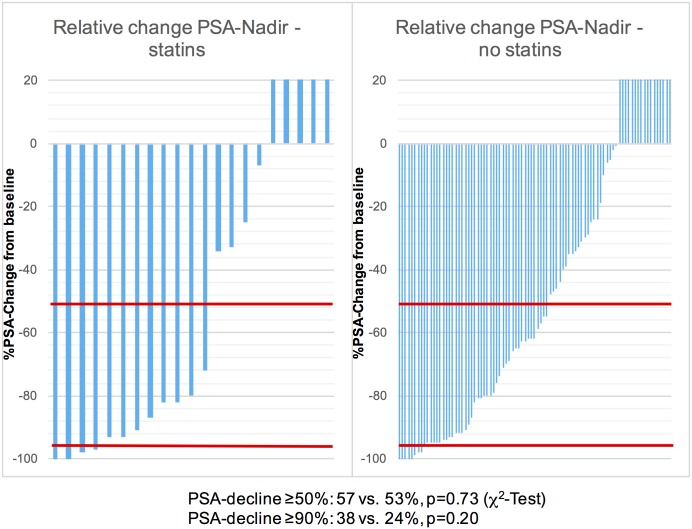
PSA-decline ≥ 50% was not significantly different in both groups (57 vs. 53%; p = 0.73). The median PFS (9 vs. 10 months; p = 0.97) and OS (14 vs. 18 months; p = 0.77) did not differ significantly between those men treated with and without concomitant statin therapy, respectively. Accordingly, there was no improvement for best clinical benefit in patients using statins (odds ratio: 1.2 (CI: 0.4-4.2); p = 0.76).
Use of statins as concomitant medication did not improve survival outcomes or best clinical benefit in men with mCRPC treated with Abiraterone.
尽管目前确切机制尚不清楚,但他汀类药物被认为可改善各种恶性肿瘤的生存结局。然而对于前列腺癌,已知他汀类药物会与脱氢表雄酮(DHEAS)竞争通过溶质载体转运体进入细胞溶质,从而减少作为雄激素前体的DHEAS的细胞摄取。阿比特龙可抑制CYP17A1,从而有效降低包括DHEAS在内的所有相关雄激素的产生。在本研究中,我们探讨了在接受阿比特龙治疗的转移性去势抵抗性前列腺癌(mCRPC)患者中,他汀类药物是否仍会影响生存结局。
对2010年2月至2015年7月期间接受阿比特龙治疗的108例mCRPC男性患者进行了研究,其中21例同时接受他汀类药物治疗,87例未接受他汀类药物治疗。采用Kaplan-Meier估计法和单因素Cox回归分析对无进展生存期(PFS)和总生存期(OS)进行分析。采用双因素和多因素逻辑回归分析阿比特龙治疗下对最佳临床获益的影响。
两组患者前列腺特异性抗原(PSA)下降≥50%的情况无显著差异(57%对53%;p = 0.73)。接受他汀类药物联合治疗和未接受联合治疗的患者,其PFS中位数(9个月对10个月;p = 0.97)和OS中位数(14个月对18个月;p = 0.77)均无显著差异。因此,使用他汀类药物的患者在最佳临床获益方面并无改善(优势比:1.2(95%置信区间:0.4 - 4.2);p = 0.76)。
在接受阿比特龙治疗的mCRPC男性患者中,使用他汀类药物作为辅助用药并不能改善生存结局或最佳临床获益。