Takiguchi Gosuke, Nakamura Tetsu, Otowa Yasunori, Tomono Ayako, Kanaji Shingo, Oshikiri Taro, Suzuki Satoshi, Ishida Tsukasa, Kakeji Yoshihiro
Division of Gastrointestinal Surgery, Department of Surgery, Kobe University Graduate School of Medicine, 7-5-2 Kusunoki-chou, Chuo-ku, Kobe, Hyogo, 650-0017, Japan.
Division of Gastroenterology, Department of Internal Medicine, Kobe University Graduate School of Medicine, Kobe, Hyogo, 650-0017, Japan.
Surg Case Rep. 2016 Dec;2(1):90. doi: 10.1186/s40792-016-0219-5. Epub 2016 Sep 2.
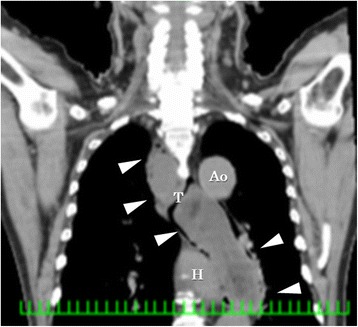
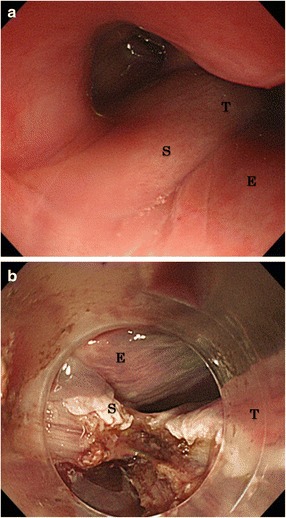
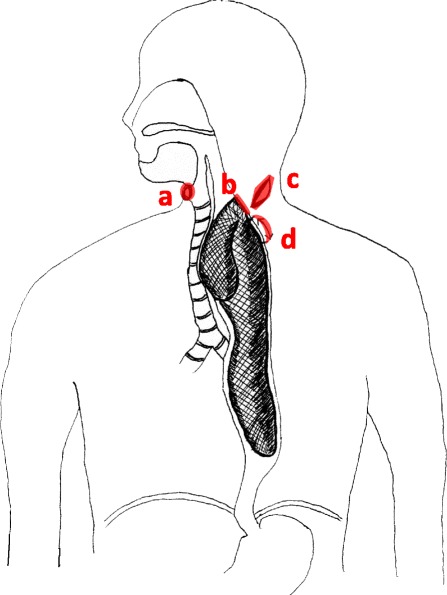
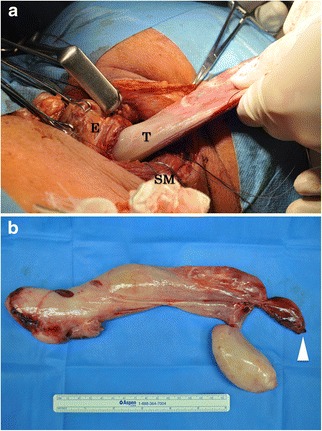
Liposarcoma of the esophagus is very rare. We experienced a huge (27.5 × 11.6 cm) liposarcoma of the esophagus. A 73-year-old man presented with severe dyspnea requiring emergency tracheal intubation. Computed tomography and esophagogastroduodenoscopy showed a large submucosal tumor arising from the esophageal entrance and extending intraluminally to the lower esophagus. We successfully performed endoscopic submucosal dissection (ESD) and esophagotomy to remove the tumor, which preserved swallowing and phonation. The final diagnosis by histopathologic and immunohistologic examination was well-differentiated liposarcoma of the esophagus. Treatment by the combination of ESD and esophagotomy can be performed even for a very large tumor. This method preserves deglutition with a lower risk of recurrent laryngeal nerve paralysis than that with esophagectomy.
食管脂肪肉瘤非常罕见。我们遇到了一例巨大的(27.5×11.6厘米)食管脂肪肉瘤。一名73岁男性因严重呼吸困难需要紧急气管插管。计算机断层扫描和食管胃十二指肠镜检查显示,一个大的黏膜下肿瘤起源于食管入口,并向腔内延伸至食管下段。我们成功地进行了内镜下黏膜下剥离术(ESD)和食管切开术以切除肿瘤,该手术保留了吞咽和发声功能。组织病理学和免疫组织学检查的最终诊断为食管高分化脂肪肉瘤。即使对于非常大的肿瘤,ESD和食管切开术联合治疗也可实施。该方法保留了吞咽功能,与食管切除术相比,喉返神经麻痹的复发风险更低。