Castleberry Anthony W, Bishawi Muath, Worni Mathias, Erhunmwunsee Loretta, Speicher Paul J, Osho Asishana A, Snyder Laurie D, Hartwig Matthew G
Department of Surgery, Division of Cardiothoracic Surgery, Duke University Medical Center, Durham, North Carolina.
Department of Surgery, Division of Cardiothoracic Surgery, Duke University Medical Center, Durham, North Carolina.
Ann Thorac Surg. 2017 Jan;103(1):274-280. doi: 10.1016/j.athoracsur.2016.06.067. Epub 2016 Sep 10.
Our objective was to identify potential avenues for resource allocation and patient advocacy to improve outcomes by evaluating the association between recipient sociodemographic and patient characteristics and medication nonadherence after lung transplantation.
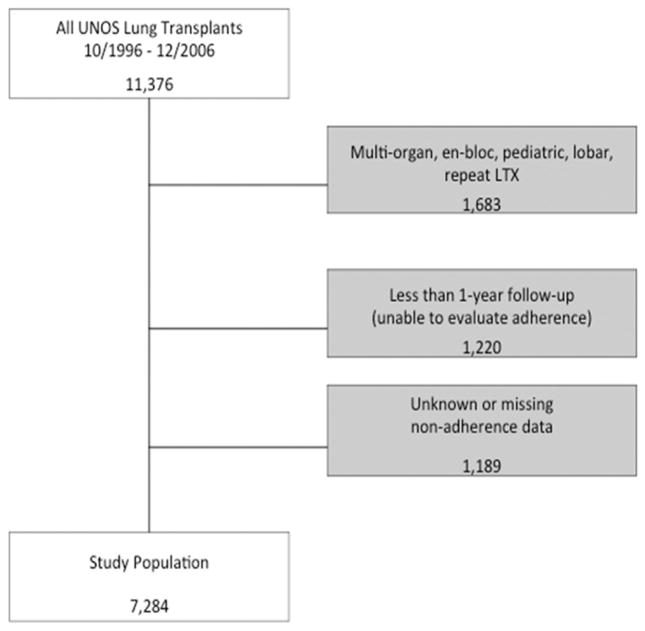
States US adult, lung-only transplantations per the United Network for Organ Sharing database were analyzed from October 1996 through December 2006, based on the period during which nonadherence information was recorded. Generalized linear models were used to determine the association of demographic, disease, and transplantation center characteristics with early nonadherence (defined as within the first year after transplantation) as well as late nonadherence (years 2 to 4 after transplantation). Outcomes comparing adherent and nonadherent patients were also evaluated.
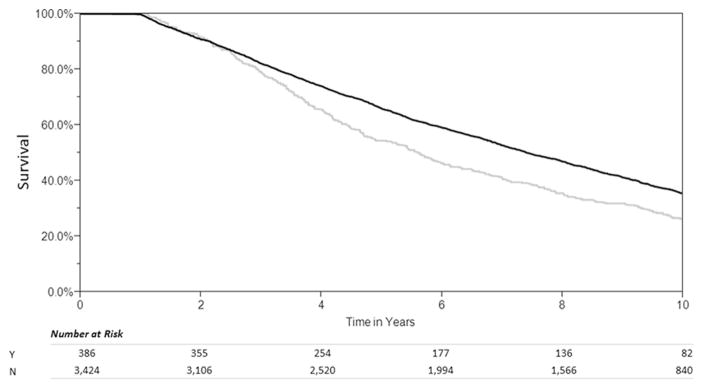
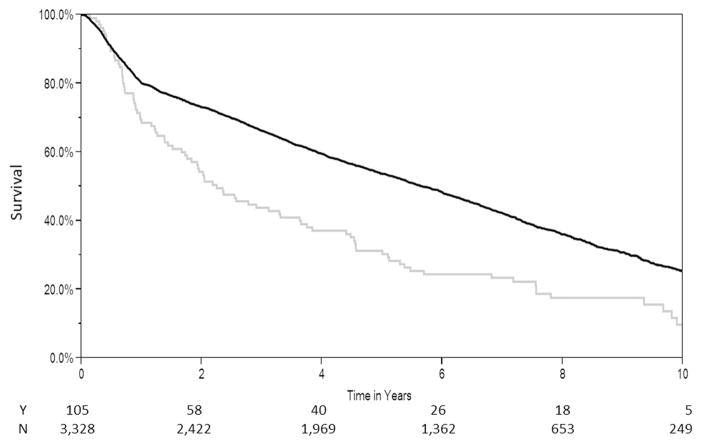
Patients (n = 7,284) were included for analysis. Early and late nonadherence rates were 3.1% and 10.6%, respectively. Factors associated with early nonadherence were Medicaid insurance compared with private insurance (adjusted odds ratio [AOR] 2.45, 95% confidence interval [CI]: 1.16 to 5.15), and black race (AOR 2.38, 95% CI: 1.08 to 5.25). Medicaid insurance and black race were also associated with late nonadherence (AOR 2.38, 95% CI: 1.51 to 3.73 and OR 1.73, 95% CI: 1.04 to 2.89, respectively), as were age 18 to 20 years (AOR 3.41, 95% CI: 1.29 to 8.99) and grade school or lower education (AOR 1.88, 95% CI: 1.05 to 3.35). Early and late nonadherence were both associated with significantly shorter unadjusted survival (p < 0.001).
Identifying patients at risk of nonadherence may enable resource allocation and patient advocacy to improve outcomes.
我们的目标是通过评估肺移植受者的社会人口统计学和患者特征与用药不依从之间的关联,确定资源分配和患者支持的潜在途径,以改善治疗结果。
根据记录不依从信息的时间段,对1996年10月至2006年12月美国器官共享联合网络数据库中的美国成年单肺移植病例进行分析。使用广义线性模型确定人口统计学、疾病和移植中心特征与早期不依从(定义为移植后第一年内)以及晚期不依从(移植后第2至4年)之间的关联。还评估了依从性和不依从性患者的治疗结果比较。
纳入分析的患者有7284例。早期和晚期不依从率分别为3.1%和10.6%。与早期不依从相关的因素包括与私人保险相比的医疗补助保险(调整后的优势比[AOR]为2.45,95%置信区间[CI]:1.16至5.15)以及黑人种族(AOR为2.38,95%CI:1.08至5.25)。医疗补助保险和黑人种族也与晚期不依从相关(AOR分别为2.38,95%CI:1.51至3.73和OR为1.73,95%CI:1.04至2.89),18至20岁的年龄(AOR为3.41,95%CI:1.29至8.99)以及小学或更低教育程度(AOR为1.88,95%CI:1.05至3.35)也与之相关。早期和晚期不依从均与未经调整的生存期显著缩短相关(p<0.001)。
识别有不依从风险的患者可能有助于资源分配和患者支持,从而改善治疗结果。