Michelet Daphnée, Andreu-Gallien Juliette, Skhiri Alia, Bonnard Arnaud, Nivoche Yves, Dahmani Souhayl
Department of Anesthesia, Intensive Care and Pain Management, Robert Debré University Hospital, Paris Diderot University, Paris, France.
Department of Pain Management and Palliative Care, Armand-Trousseau University Hospital, Paris Pierre et Marie Curie University, Paris, France.
J Anaesthesiol Clin Pharmacol. 2016 Jul-Sep;32(3):369-75. doi: 10.4103/0970-9185.168196.
Laparoscopic pediatric surgery allows a rapid postoperative rehabilitation and hospital discharge. However, the optimal postoperative pain management preserving advantages of this surgical technique remains to be determined. This study aimed to identify factors affecting the postoperative recovery of bowel function after laparoscopic surgery in children.
A retrospective analysis of factors affecting recovery of bowel function in children and infants undergoing laparoscopic surgery between January 1, 2009 and September 30, 2009, was performed. Factors included were: Age, weight, extent of surgery (extensive, regional or local), chronic pain (sickle cell disease or chronic intestinal inflammatory disease), American Society of Anaesthesiologists status, postoperative analgesia (ketamine, morphine, nalbuphine, paracetamol, nonsteroidal anti-inflammatory drugs [NSAIDs], nefopam, regional analgesia) both in the Postanesthesia Care Unit and in the surgical ward; and surgical complications. Data analysis used classification and regression tree analysis (CART) with a 10-fold cross validation.
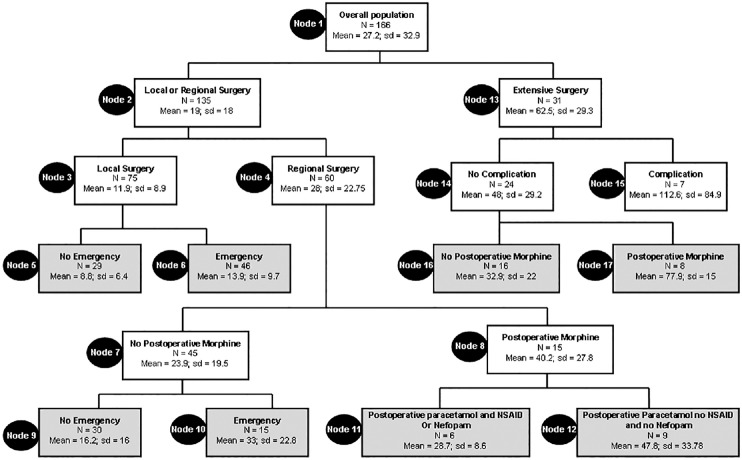
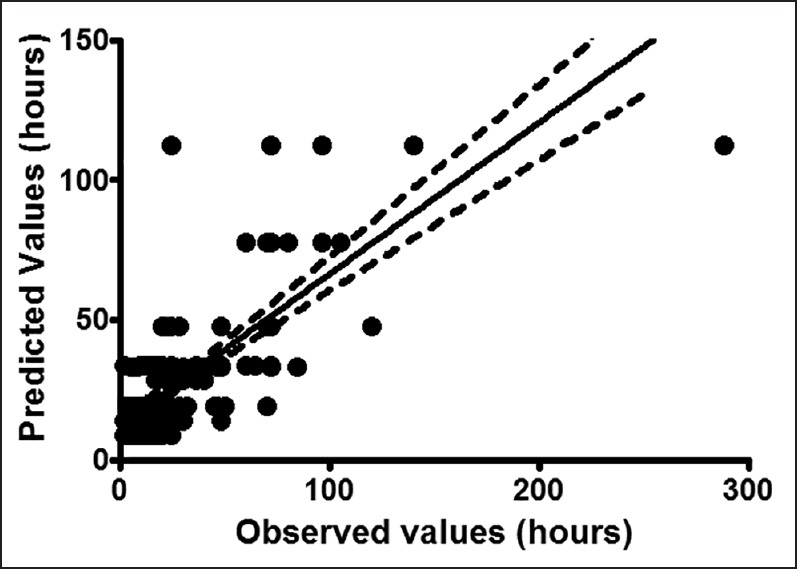
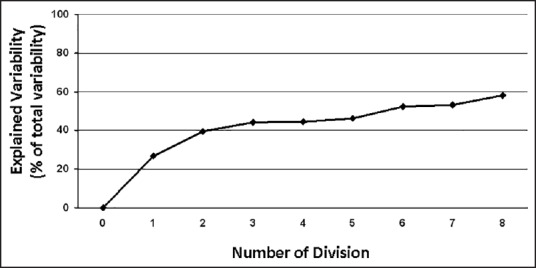
One hundred and sixty six patients were included in the analysis. Recovery of bowel function depended upon: The extent of surgery, the occurrence of postoperative surgical complications, the administration of postoperative morphine in the surgical ward, the coadministration of paracetamol and NSAIDs and/or nefopam in the surgical ward and the emergency character of the surgery. The CART method generated a decision tree with eight terminal nodes. The percentage of explained variability of the model and the cross validation were 58% and 49%, respectively.
Multimodal analgesia using nonopioid analgesia that allows decreasing postoperative morphine consumption should be considered for the speed of bowel function recovery after laparoscopic pediatric surgery.
小儿腹腔镜手术可使患者术后快速康复并出院。然而,能保留该手术技术优势的最佳术后疼痛管理方案仍有待确定。本研究旨在确定影响小儿腹腔镜手术后肠功能恢复的因素。
对2009年1月1日至2009年9月30日期间接受腹腔镜手术的儿童和婴儿肠功能恢复的影响因素进行回顾性分析。纳入的因素包括:年龄、体重、手术范围(广泛、局部或区域)、慢性疼痛(镰状细胞病或慢性肠道炎症性疾病)、美国麻醉医师协会分级、麻醉后护理单元及外科病房的术后镇痛(氯胺酮、吗啡、纳布啡、对乙酰氨基酚、非甾体类抗炎药[NSAIDs]、奈福泮、区域镇痛);以及手术并发症。数据分析采用分类与回归树分析(CART)并进行10倍交叉验证。
166例患者纳入分析。肠功能的恢复取决于:手术范围、术后手术并发症的发生、外科病房术后吗啡的使用、外科病房对乙酰氨基酚与NSAIDs和/或奈福泮的联合使用以及手术的急诊性质。CART方法生成了一个具有八个终端节点的决策树。模型的可解释变异百分比和交叉验证分别为58%和49%。
小儿腹腔镜手术后,为促进肠功能恢复,应考虑使用非阿片类镇痛的多模式镇痛,以减少术后吗啡用量。