Peng Qin, Li Kang, Cao Ming Rong, Bie Cai Qun, Tang Hui Jun, Tang Shao Hui
Department of Gastroenterology, The First Affiliated Hospital, Jinan University, 613 Huang Pu Avenue, Guangzhou, China.
Department of Gastroenterology, The Affiliated HeXian Memorial Hospital, Southern Medical University, Guangzhou, China.
Springerplus. 2016 Sep 15;5(1):1569. doi: 10.1186/s40064-016-3218-x. eCollection 2016.
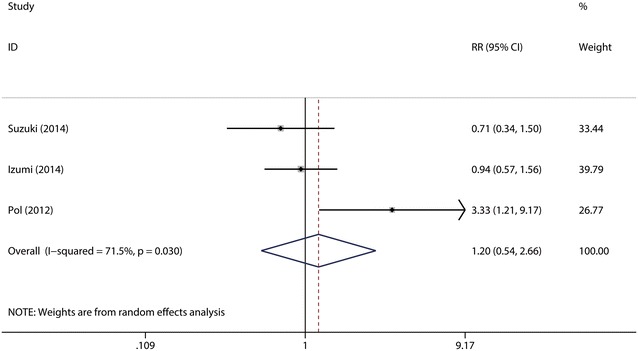
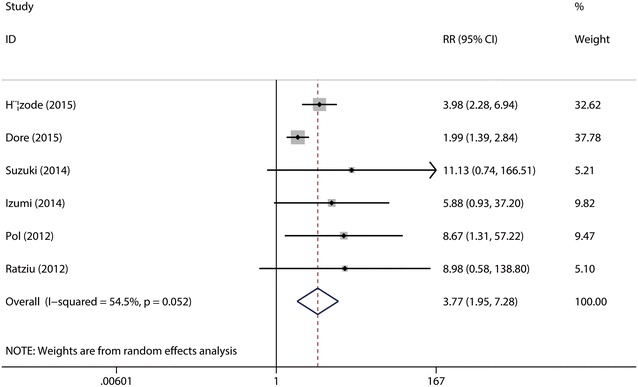
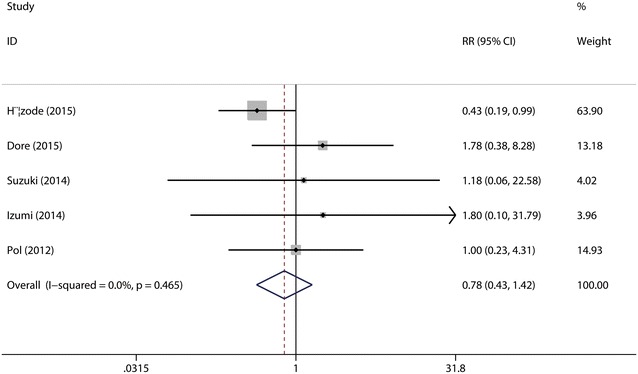
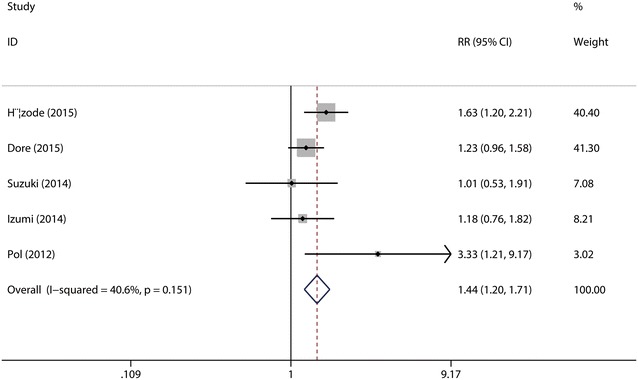
Daclatasvir, a HCV NS5A inhibitor, is a new direct-acting antiviral drug for chronic hepatitis C (CHC). This study aimed to evaluate the efficacy and safety of daclatasvir combined with peginterferon-α (pegIFN-α) and ribavirin (RBV) for the treatment of CHC. The databases of PUBMED, EMBASE, COCHRANE, WANFANG, and CNKI were retrieved to identify eligible studies. Pooled risk ratio (RR) and 95 % confidence interval (CI) were calculated using random or fixed models. A total of six RCTs including 1100 adult patients with CHC met the inclusion criteria and the patients were infected with HCV genotype 1-4, with the genotype 1 infection accounting for 73.1 %. Meta-analysis showed daclatasvir-based combination therapy yielded a significantly higher probability of achieving the overall RVR (46.43 vs. 18.97 %) with pooled RR of 3.77 (95 % CI 1.95-7.28, p < 0.0001) and a slightly higher probability of achieving the overall SVR24 (65.08 vs. 47.77 %) with pooled RR of 1.41 (95 % CI 1.18-1.68, p < 0.0001), and did not show increased adverse events compared with the pegIFN-α/RBV regimen (control group). Subgroup analysis showed the rate of RVR and SVR24 in high-dose daclatasvir (60 mg/day) group were slightly higher than the overall results; the rate of RVR in low-dose daclatasvir (10 mg/day) group was also higher than the control group, but its SVR24 rate was similar between the two groups. Daclatasvir combined with pegIFN-α/RBV is effective and safe in treating adult patients with CHC, especially HCV genotype 1 infection, and daclatasvir (60 mg/day) is a better choice as compared with daclatasvir (10 mg/day).
达卡他韦是一种丙型肝炎病毒(HCV)NS5A抑制剂,是一种用于治疗慢性丙型肝炎(CHC)的新型直接抗病毒药物。本研究旨在评估达卡他韦联合聚乙二醇干扰素-α(pegIFN-α)和利巴韦林(RBV)治疗CHC的疗效和安全性。检索了PUBMED、EMBASE、COCHRANE、万方和知网数据库以确定符合条件的研究。使用随机或固定模型计算合并风险比(RR)和95%置信区间(CI)。共有6项随机对照试验(RCT)纳入了1100例成年CHC患者,这些患者感染了HCV 1-4型,其中1型感染占73.1%。荟萃分析显示,基于达卡他韦的联合治疗实现总体快速病毒学应答(RVR)的概率显著更高(46.43%对18.97%),合并RR为3.77(95%CI 1.95-7.28,p<0.0001),实现总体治疗结束后24周持续病毒学应答(SVR24)的概率略高(65.08%对47.77%),合并RR为1.41(95%CI 1.18-1.68,p<0.0001),并且与聚乙二醇干扰素-α/利巴韦林方案(对照组)相比,未显示不良事件增加。亚组分析显示,高剂量达卡他韦(60mg/天)组的RVR和SVR24率略高于总体结果;低剂量达卡他韦(10mg/天)组的RVR率也高于对照组,但其SVR24率在两组之间相似。达卡他韦联合聚乙二醇干扰素-α/利巴韦林治疗成年CHC患者有效且安全,尤其是HCV 1型感染患者,与达卡他韦(10mg/天)相比,达卡他韦(6mg/天)是更好的选择。