Dervan Andrew P, Deverka Patricia A, Trosman Julia R, Weldon Christine B, Douglas Michael P, Phillips Kathryn A
Division of Medical Genetics, Department of Medicine, University of Washington, Seattle, Washington, USA.
American Institutes for Health Research and Innovation, Chapel Hill, North Carolina, USA.
Genet Med. 2017 May;19(5):559-567. doi: 10.1038/gim.2016.145. Epub 2016 Sep 22.
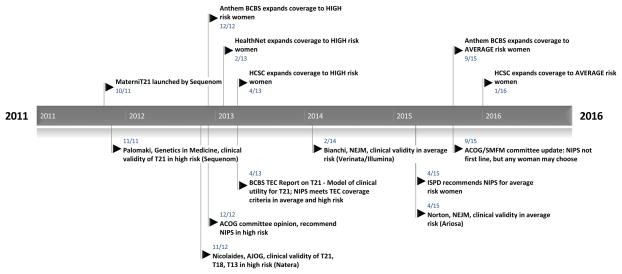
Cell-free DNA (cfDNA) prenatal screening tests have been rapidly adopted into clinical practice, due in part to positive insurance coverage. We evaluated the framework payers used in making coverage decisions to describe a process that should be informative for other sequencing tests.
We analyzed coverage policies from the 19 largest US private payers with publicly available policies through February 2016, building from the University of California San Francisco TRANSPERS Payer Coverage Policy Registry.
All payers studied cover cfDNA screening for detection of trisomies 21, 18, and 13 in high-risk, singleton pregnancies, based on robust clinical validity (CV) studies and modeled evidence of clinical utility (CU). Payers typically evaluated the evidence for each chromosomal abnormality separately, although results are offered as part of a panel. Starting in August 2015, 8 of the 19 payers also began covering cfDNA screening in average-risk pregnancies, citing recent CV studies and updated professional guidelines. Most payers attempted, but were unable, to independently assess analytic validity (AV).
Payers utilized the standard evidentiary framework (AV/CV/CU) when evaluating cfDNA screening but varied in their interpretation of the sufficiency of the evidence. Professional guidelines, large CV studies, and decision analytic models regarding health outcomes appeared highly influential in coverage decisions.Genet Med advance online publication 22 September 2016.
游离DNA(cfDNA)产前筛查检测已迅速应用于临床实践,部分原因是保险覆盖范围良好。我们评估了支付方用于做出覆盖范围决策的框架,以描述一个对其他测序检测有参考价值的过程。
我们分析了截至2016年2月美国19家最大的具有公开可用政策的私人支付方的覆盖政策,这些政策来自加利福尼亚大学旧金山分校的TRANSPERS支付方覆盖政策登记处。
基于有力的临床有效性(CV)研究和临床效用(CU)的模型证据,所有研究的支付方都覆盖了对高危单胎妊娠中21、18和13三体的cfDNA筛查。支付方通常分别评估每种染色体异常的证据,尽管结果是作为一个检测组合的一部分提供的。从2015年8月开始,19家支付方中有8家也开始覆盖平均风险妊娠的cfDNA筛查,理由是最近的CV研究和更新的专业指南。大多数支付方试图但无法独立评估分析有效性(AV)。
支付方在评估cfDNA筛查时采用了标准的证据框架(AV/CV/CU),但在对证据充分性的解释上存在差异。专业指南、大型CV研究以及关于健康结果的决策分析模型在覆盖范围决策中似乎具有很大影响力。《遗传医学》于2016年9月22日在线优先发表。