Lee Hyo Jin, Choi Jae Ki, Cho Sung Yeon, Kim Si Hyun, Park Sun Hee, Choi Su Mi, Lee Dong Gun, Choi Jung Hyun, Yoo Jin Hong
Division of Infectious Diseases, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Vaccine Bio Research Institute, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Infect Chemother. 2016 Sep;48(3):166-173. doi: 10.3947/ic.2016.48.3.166. Epub 2016 Sep 8.
Carbapenemase-producing Enterobacteriaceae (CPE) are Gram-negative bacteria with increasing prevalence of infection worldwide. In Korea, 25 cases of CPE isolates were reported by the Korea Centers for Disease Control and Prevention in 2011. Most CPE cases were detected mainly at tertiary referral hospitals. We analyzed the prevalence and risk factors for carbapenem-resistant Enterobacteriaceae (CRE) in a mid-sized community-based hospital in Korea.
We retrospectively analyzed all consecutive episodes of Enterobacteriaceae in a mid-sized community-based hospital from January 2013 to February 2014. CRE was defined as organisms of Enterobacteriaceae showing decreased susceptibility to carbapenems. Risk factors for CRE were evaluated by a case-double control design. Carbapenemase was confirmed for CRE using a combined disc test.
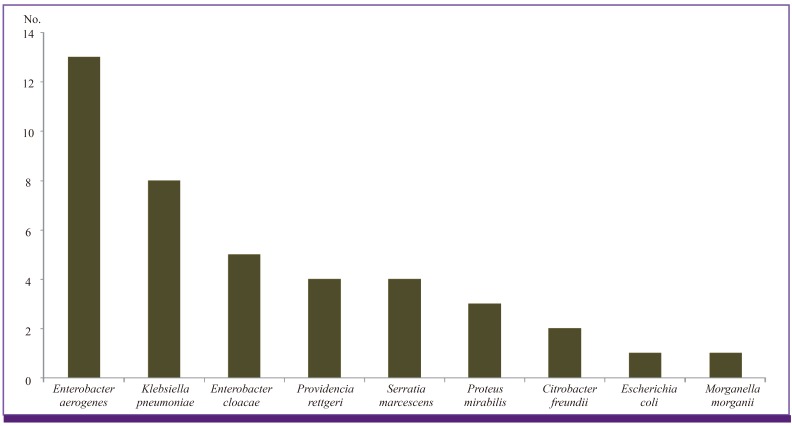
During 229,710 patient-days, 2,510 Enterobacteriaceae isolates were obtained. A total of 41 (1.6%) CRE isolates were enrolled in the study period. Thirteen species (31.7%) were Enterobacter aerogenes, 8 (19.5%) Klebsiella pneumoniae, 5 (12.2%) Enterobacter cloacae, and 15 other species of Enterobacteriaceae, respectively. Among the 41 isolates, only one (2.4%) E. aerogenes isolate belonged to CPE. For evaluation of risk factors, a total of 111 patients were enrolled and this included 37 patients in the CRE group, 37 in control group I (identical species), and 37 in control group II (different species). Based on multivariate analysis, regularly visiting the outpatient clinic was a risk factor for CRE acquisition in the control group I (P = 0.003), while vascular catheter and Charlson comorbidity index score ≥ 3 were risk factors in control group II (P = 0.010 and 0.011, each). Patients with CRE were more likely to experience a reduced level of consciousness, use a vasopressor, be under intensive care, and suffer from acute kidney injury. However, CRE was not an independent predictor of mortality compared with both control groups.
In conclusion, the prevalence of CRE was higher than expected in a mid-sized community-based hospital in Korea. CRE should be considered when patients have a vascular catheter, high comorbidity score, and regular visits to the outpatient clinic. This study suggests the need for appropriate prevention efforts and constant attention to CRE infection control in a mid-sized community-based hospital.
产碳青霉烯酶肠杆菌科细菌(CPE)是革兰氏阴性菌,在全球范围内感染的患病率不断上升。2011年,韩国疾病控制与预防中心报告了25例CPE分离株。大多数CPE病例主要在三级转诊医院被检测到。我们分析了韩国一家中型社区医院中产碳青霉烯类耐药肠杆菌科细菌(CRE)的患病率及危险因素。
我们回顾性分析了2013年1月至2014年2月一家中型社区医院中所有连续发生的肠杆菌科感染病例。CRE被定义为对碳青霉烯类药物敏感性降低的肠杆菌科细菌。通过病例对照双因素设计评估CRE的危险因素。使用复合纸片法确认CRE是否产碳青霉烯酶。
在229,710个患者日期间,共获得2,510株肠杆菌科细菌分离株。在研究期间,共纳入41株(1.6%)CRE分离株。其中13株(31.7%)为产气肠杆菌,8株(19.5%)为肺炎克雷伯菌,5株(12.2%)为阴沟肠杆菌,其余15株为其他肠杆菌科细菌。在这41株分离株中,只有1株(2.4%)产气肠杆菌分离株属于CPE。为评估危险因素,共纳入111例患者,其中CRE组37例,对照组I(相同菌种)37例,对照组II(不同菌种)37例。基于多因素分析,在对照组I中,定期到门诊就诊是获得CRE的危险因素(P = 0.003),而在对照组II中,血管导管及Charlson合并症指数评分≥3是危险因素(分别为P = 0.010和0.011)。CRE患者更易出现意识水平降低、使用血管活性药物、入住重症监护病房及发生急性肾损伤。然而,与两个对照组相比,CRE并非死亡的独立预测因素。
总之,在韩国一家中型社区医院中,CRE的患病率高于预期。当患者有血管导管、高合并症评分及定期到门诊就诊时,应考虑CRE感染。本研究表明,在中型社区医院中需要采取适当的预防措施并持续关注CRE感染控制。