Doepker Matthew P, Yamamoto Maki, Applebaum Matthew A, Patel Nupur U, Jaime Montilla-Soler M, Sarnaik Amod A, Wayne Cruse C, Sondak Vernon K, Zager Jonathan S
Department of Cutaneous Oncology, Moffitt Cancer Center, Tampa, FL, USA.
Department of Surgery, University of California Irvine Medical Center, Orange, CA, USA.
Ann Surg Oncol. 2017 Feb;24(2):355-361. doi: 10.1245/s10434-016-5590-8. Epub 2016 Sep 22.
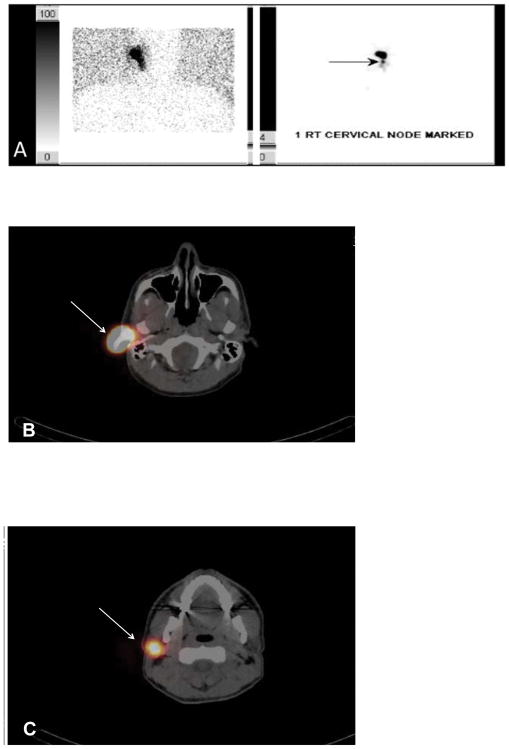
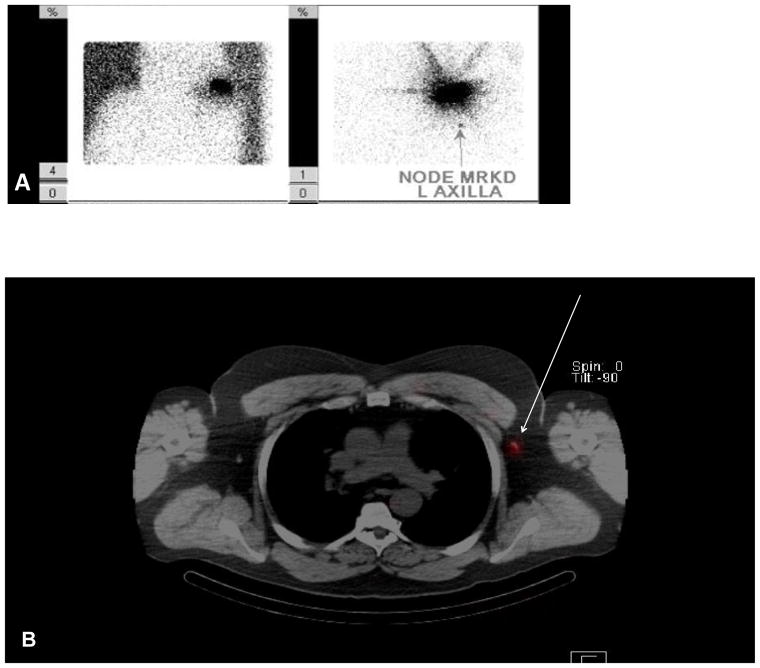
Accurate preoperative lymphoscintigraphy is vital to performing sentinel lymph node biopsy (SLNB) for cutaneous malignancies. Potential advantages of single-photon emission computed tomography with integrated computed tomography (SPECT/CT) include the ability to readily identify aberrant drainage patterns as well as provide the surgeon with three-dimensional anatomic landmarks not seen on conventional planar lymphoscintigraphy (PLS).
Patients with cutaneous malignancies who underwent SLNB with preoperative imaging using both SPECT/CT and PLS from 2011 to 2014 were identified.
Both SPECT/CT and PLS were obtained in 351 patients (median age, 69 years; range, 5-94 years) with cutaneous malignancies (melanoma = 300, Merkel cell carcinoma = 33, squamous cell carcinoma = 8, other = 10) after intradermal injection of technetium sulfur colloid (median dose 300 µCi). A mean of 4.3 hot spots were identified on SPECT/CT compared to 3.0 on PLS (p < 0.001). One hundred fifty-three patients (43.6 %) had identical findings between SPECT/CT and PLS, while 172 (49 %) had additional hot spots identified on SPECT/CT compared to only 24 (6.8 %) additional on PLS. SPECT/CT demonstrated additional nodal basins in 103 patients (29.4 %), compared to only 11 patients (3.1 %) with additional basins on PLS.
SPECT/CT is a useful adjunct that can help with sentinel node localization in challenging cases. It identified additional hot spots not seen on PLS in almost 50 % of patients. Because PLS identified hot spots not seen on SPECT/CT in 6.8 % of patients, we recommend using both modalities jointly. Long-term follow-up will be required to validate the clinical significance of the additional hot spots identified by SPECT/CT.
准确的术前淋巴闪烁显像对于皮肤恶性肿瘤前哨淋巴结活检(SLNB)至关重要。单光子发射计算机断层扫描与计算机断层扫描融合技术(SPECT/CT)的潜在优势包括能够轻松识别异常引流模式,并为外科医生提供传统平面淋巴闪烁显像(PLS)无法看到的三维解剖标志。
确定2011年至2014年期间接受SLNB且术前使用SPECT/CT和PLS成像的皮肤恶性肿瘤患者。
351例皮肤恶性肿瘤患者(中位年龄69岁;范围5 - 94岁)(黑色素瘤300例、默克尔细胞癌33例、鳞状细胞癌8例、其他10例)在皮内注射硫化锝胶体(中位剂量300μCi)后接受了SPECT/CT和PLS检查。SPECT/CT平均识别出4.3个热点,而PLS为3.0个(p < 0.001)。153例患者(43.6%)SPECT/CT和PLS结果相同,172例(49%)患者SPECT/CT识别出额外热点,而PLS仅额外识别出24例(6.8%)。SPECT/CT显示103例患者(29.4%)有额外的淋巴结区域,而PLS仅显示11例患者(3.1%)有额外区域。
SPECT/CT是一种有用的辅助手段,可帮助在具有挑战性的病例中进行前哨淋巴结定位。它在近50%的患者中识别出PLS未发现的额外热点。由于6.8%的患者PLS识别出SPECT/CT未发现的热点,我们建议联合使用这两种方法。需要长期随访以验证SPECT/CT识别出的额外热点的临床意义。