Cheng Shun-Yang, Chou Yu-Hsiang, Liao Fang-Ling, Lin Chi-Chun, Chang Fan-Chi, Liu Chia-Hao, Huang Tao-Min, Lai Chun-Fu, Lin Yu-Feng, Wu Vin-Cent, Chu Tzong-Shinn, Wu Ming-Shiou, Lin Shuei-Liong
Graduate Institute of Physiology, College of Medicine, National Taiwan University, Taipei, Taiwan.
Renal Division, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan.
Sci Rep. 2016 Sep 28;6:34265. doi: 10.1038/srep34265.
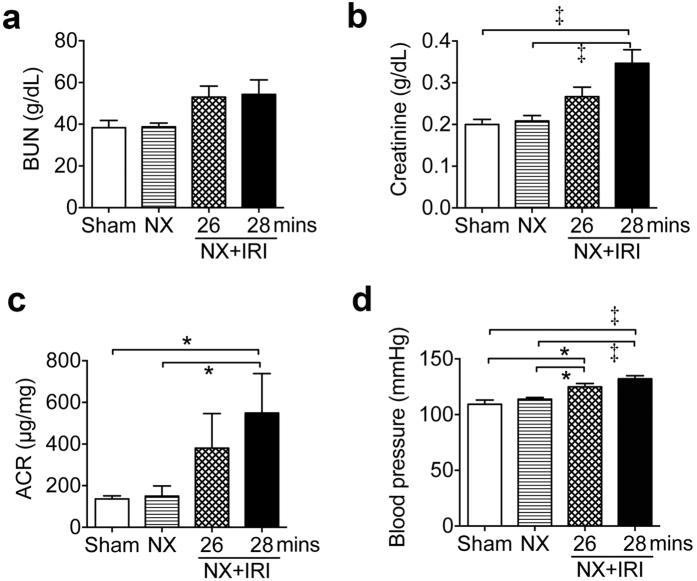
Acute kidney injury (AKI) is an important risk factor for incident chronic kidney disease (CKD). Clinical studies disclose that ensuing CKD progresses after functional recovery from AKI, but the underlying mechanisms remain illusive. Using a murine model representing AKI-CKD continuum, we show angiotensin II type 1a (AT1a) receptor signaling as one of the underlying mechanisms. Male adult CD-1 mice presented severe AKI with 20% mortality within 2 weeks after right nephrectomy and left renal ischemia-reperfusion injury. Despite functional recovery, focal tubular atrophy, interstitial cell infiltration and fibrosis, upregulation of genes encoding angiotensinogen and AT1a receptor were shown in kidneys 4 weeks after AKI. Thereafter mice manifested increase of blood pressure, albuminuria and azotemia progressively. Drinking water with or without losartan or hydralazine was administered to mice from 4 weeks after AKI. Increase of mortality, blood pressure, albuminuria, azotemia and kidney fibrosis was noted in mice with vehicle administration during the 5-month experimental period. On the contrary, these parameters in mice with losartan administration were reduced to the levels shown in control group. Hydralazine did not provide similar beneficial effect though blood pressure was controlled. These findings demonstrate that losartan can reduce ensuing CKD and mortality after functional recovery from AKI.
急性肾损伤(AKI)是新发慢性肾脏病(CKD)的一个重要危险因素。临床研究表明,AKI后发生的CKD在功能恢复后仍会进展,但其潜在机制仍不清楚。利用一个代表AKI-CKD连续过程的小鼠模型,我们发现1a型血管紧张素II(AT1a)受体信号传导是潜在机制之一。雄性成年CD-1小鼠在右肾切除和左肾缺血再灌注损伤后2周内出现严重AKI,死亡率为20%。尽管功能恢复,但在AKI后4周,小鼠肾脏出现局灶性肾小管萎缩、间质细胞浸润和纤维化,血管紧张素原和AT1a受体编码基因上调。此后,小鼠逐渐出现血压升高、蛋白尿和氮质血症。从AKI后4周开始,给小鼠饮用含或不含氯沙坦或肼屈嗪的水。在5个月的实验期内,给予载体的小鼠死亡率、血压、蛋白尿、氮质血症和肾纤维化增加。相反,给予氯沙坦的小鼠的这些参数降至对照组所示水平。尽管血压得到控制,但肼屈嗪没有提供类似的有益效果。这些发现表明,氯沙坦可以降低AKI功能恢复后发生的CKD及死亡率。