Peters Esther, Mehta Ravindra L, Murray Patrick T, Hummel Jürgen, Joannidis Michael, Kellum John A, Arend Jacques, Pickkers Peter
Department of Intensive Care Medicine, Radboud university medical center, Nijmegen, The Netherlands Department of Pharmacology and Toxicology, Radboud university medical center, Nijmegen, The Netherlands.
Division of Nephrology, Department of Medicine, University of California, San Diego, California, USA.
BMJ Open. 2016 Sep 27;6(9):e012371. doi: 10.1136/bmjopen-2016-012371.
Acute kidney injury (AKI) occurs in 55-60% of critically ill patients, and sepsis is the most common underlying cause. No pharmacological treatment options are licensed to treat sepsis-associated AKI (SA-AKI); only supportive renal replacement therapy (RRT) is available. One of the limited number of candidate compounds in clinical development to treat SA-AKI is alkaline phosphatase (AP). The renal protective effect of purified bovine intestinal AP has been demonstrated in critically ill sepsis patients. To build on these observations, a human recombinant AP (recAP) was developed, of which safety and efficacy in patients with SA-AKI will be investigated in this trial.
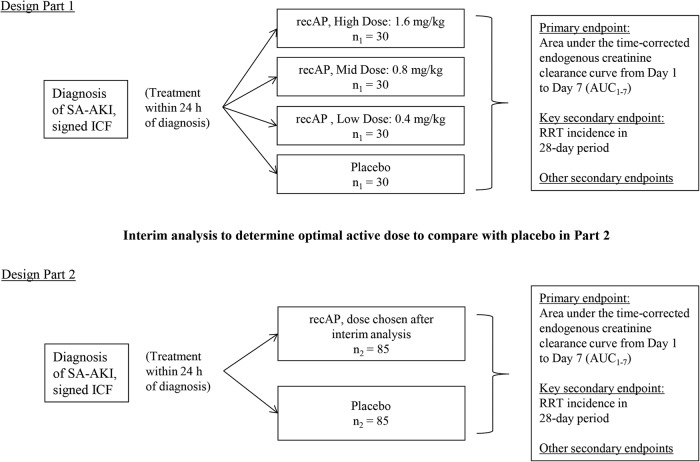
This is a randomised, double-blind, placebo-controlled, 4-arm, proof-of-concept, dose-finding adaptive phase IIa/IIb study, conducted in critically ill patients with SA-AKI. A minimum of 290 patients will be enrolled at ∼50 sites in the European Union and North America. The study involves 2 parts. Patients enrolled during Part 1 will be randomly assigned to receive either placebo (n=30) or 1 of 3 different doses of recAP (n=30 per group) once daily for 3 days (0.4, 0.8 or 1.6 mg/kg). In Part 2, patients will be randomly assigned to receive the most efficacious dose of recAP (n=85), selected during an interim analysis, or placebo (n=85). Treatment must be administered within 24 hours after SA-AKI is first diagnosed and within 96 hours from first diagnosis of sepsis. The primary end point is the area under the time-corrected endogenous creatinine clearance curve from days 1 to 7. The key secondary end point is RRT incidence during days 1-28.
This study is approved by the relevant institutional review boards/independent ethics committees and is conducted in accordance with the ethical principles of the Declaration of Helsinki, guidelines of Good Clinical Practice, Code of Federal Regulations and all other applicable regulations. Results of this study will reveal the efficacy of recAP for the improvement of renal function in critically ill patients with SA-AKI and will be published in a peer-reviewed scientific journal.
NCT02182440; Pre-results.
55%至60%的重症患者会发生急性肾损伤(AKI),脓毒症是最常见的潜在病因。目前尚无获批用于治疗脓毒症相关急性肾损伤(SA-AKI)的药物治疗方案;仅有支持性肾脏替代治疗(RRT)可用。正在进行临床开发的用于治疗SA-AKI的少数候选化合物之一是碱性磷酸酶(AP)。纯化的牛小肠AP对重症脓毒症患者的肾脏保护作用已得到证实。基于这些观察结果,开发了一种重组人AP(recAP),本试验将研究其在SA-AKI患者中的安全性和有效性。
这是一项随机、双盲、安慰剂对照、四臂、概念验证、剂量探索性适应性IIa/IIb期研究,在患有SA-AKI的重症患者中进行。在欧盟和北美的约50个地点至少招募290名患者。该研究包括2个部分。第1部分招募的患者将被随机分配,每天接受一次安慰剂(n = 30)或3种不同剂量recAP中的一种(每组n = 30),共3天(0.4、0.8或1.6mg/kg)。在第2部分,患者将被随机分配接受在中期分析中选择的最有效剂量的recAP(n = 85)或安慰剂(n = 85)。治疗必须在SA-AKI首次诊断后24小时内且在脓毒症首次诊断后96小时内进行。主要终点是第1至7天经时间校正的内源性肌酐清除率曲线下面积。关键次要终点是第1至28天的RRT发生率。
本研究已获得相关机构审查委员会/独立伦理委员会的批准,并按照《赫尔辛基宣言》的伦理原则、《药物临床试验质量管理规范》指南、《联邦法规法典》及所有其他适用法规进行。本研究结果将揭示recAP对改善SA-AKI重症患者肾功能的疗效,并将发表在同行评审的科学期刊上。
NCT02182440;预结果。