Lefèvre Gilbert, Callegari Francesca, Gsteiger Sandro, Xiong Yuan
WSJ-386.12.48.10, Novartis Institutes for Biomedical Research, Translational Medicine, Clinical PK/PD, 4002, Basel, Switzerland.
Novartis Pharma AG, 4002, Basel, Switzerland.
Drugs Aging. 2016 Oct;33(10):725-736. doi: 10.1007/s40266-016-0405-y.
The glomerular filtration rate (GFR), a measure of renal function, decreases by approximately 10 mL/min every 10 years after the age of 40 years, which could lead to the accumulation of drugs and/or renal toxicity. Pharmacokinetic studies of drugs excreted both renally and non-renally are desirable in patients with impaired renal function, defined by parameters including estimated GFR (eGFR) and creatinine clearance (CL).
We describe here a population pharmacokinetic analysis of the possible effects of renal impairment on steady-state plasma concentrations of rivastigmine and its metabolite NAP226-90 after rivastigmine patch (5 cm [4.6 mg/24 h], 10 cm [9.5 mg/24 h], 15 cm [13.3 mg/24 h], and 20 cm [17.4 mg/24 h]) and capsule (1.5, 3, 4.5, and 6 mg/12 h) treatment in patients with Alzheimer's disease.
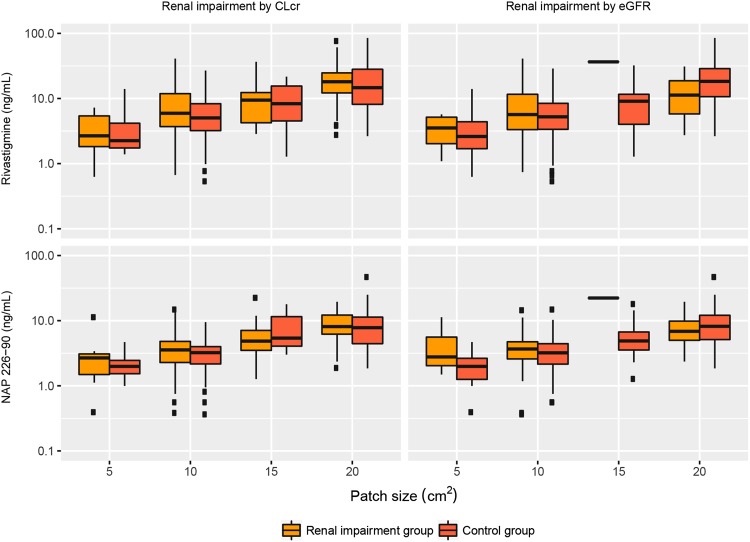
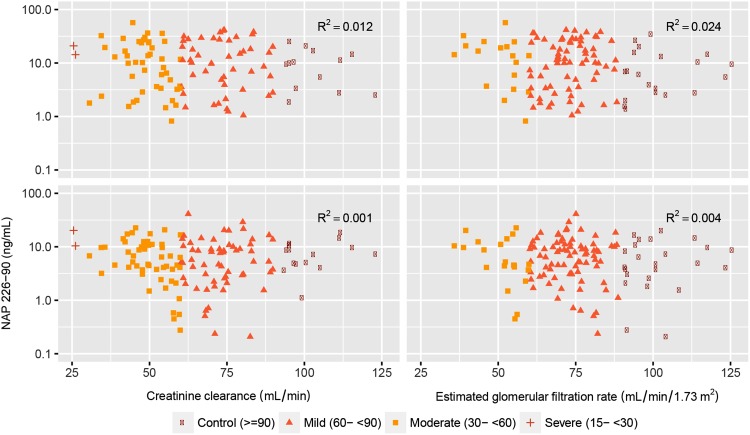
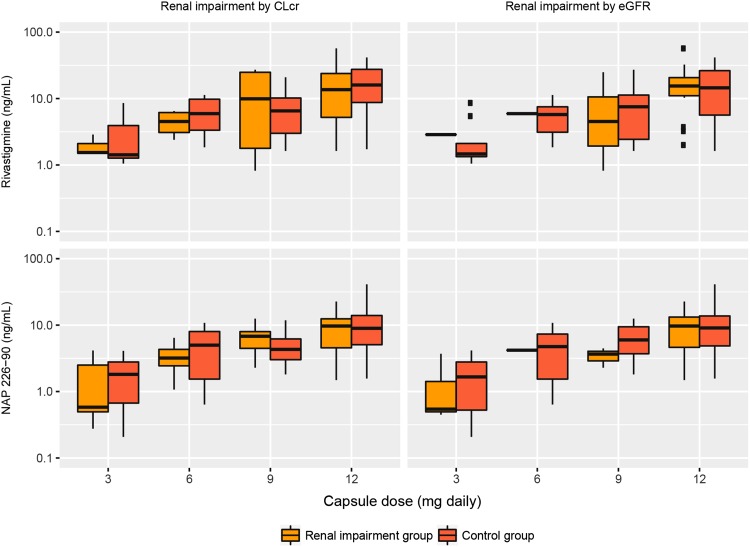
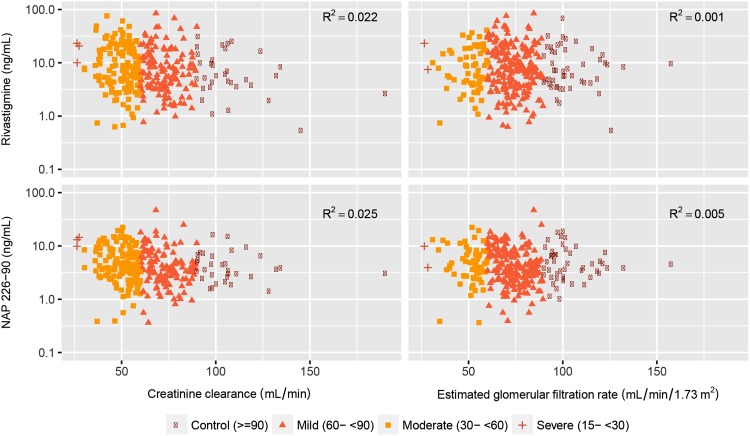
The data used to conduct the current pharmacokinetic analysis were obtained from the pivotal phase III, 24-week, multicenter, randomized, double-blind, placebo- and active-controlled, parallel-group study (IDEAL). One blood sample was collected from each patient at steady-state to measure plasma concentrations of rivastigmine and NAP226-90 using a liquid chromatography-tandem mass spectrometry (LC-MS/MS) method. The steady-state plasma concentrations of rivastigmine and NAP226-90 were plotted against CL and eGFR data, and boxplots were constructed after stratification by renal function.
The two groups (mild/no renal impairment vs. moderate/severe/end-stage renal impairment) showed comparable demographic covariates for all patch sizes and capsule doses. No correlation was observed between CL or eGFR and plasma concentrations of rivastigmine or NAP226-90. Boxplots of concentrations of rivastigmine or NAP226-90 for each dose largely overlapped for patch and capsule. Additionally, model-based estimates of plasma concentrations adjusted for body weight yielded similar results.
The results of this study show that renal function does not affect rivastigmine or NAP226-90 steady-state plasma concentrations, and no dose adjustment in patients with renal impairment is required. CLINICALTRIALS.GOV: NCT00099242.
肾小球滤过率(GFR)是衡量肾功能的指标,40岁以后每10年约下降10 mL/分钟,这可能导致药物蓄积和/或肾毒性。对于肾功能受损(由包括估算肾小球滤过率(eGFR)和肌酐清除率(CL)等参数定义)的患者,进行经肾和非经肾排泄药物的药代动力学研究很有必要。
我们在此描述一项群体药代动力学分析,探讨肾功能损害对阿尔茨海默病患者使用卡巴拉汀贴剂(5 cm [4.6 mg/24小时]、10 cm [9.5 mg/24小时]、15 cm [13.3 mg/24小时]和20 cm [17.4 mg/24小时])及胶囊(1.5、3、4.5和6 mg/12小时)治疗后卡巴拉汀及其代谢产物NAP226 - 90稳态血浆浓度的可能影响。
用于进行当前药代动力学分析的数据来自关键的III期、24周、多中心、随机、双盲、安慰剂和活性对照、平行组研究(IDEAL)。在稳态时从每位患者采集一份血样,使用液相色谱 - 串联质谱(LC - MS/MS)法测量卡巴拉汀和NAP226 - 90的血浆浓度。将卡巴拉汀和NAP226 - 90的稳态血浆浓度与CL和eGFR数据作图,并按肾功能分层后构建箱线图。
两组(轻度/无肾功能损害与中度/重度/终末期肾功能损害)在所有贴剂尺寸和胶囊剂量下的人口统计学协变量具有可比性。未观察到CL或eGFR与卡巴拉汀或NAP226 - 90血浆浓度之间存在相关性。各剂量的卡巴拉汀或NAP226 - 90浓度箱线图在贴剂和胶囊之间大部分重叠。此外,基于体重调整的血浆浓度模型估计产生了相似的结果。
本研究结果表明,肾功能不影响卡巴拉汀或NAP226 - 90稳态血浆浓度,肾功能受损患者无需调整剂量。临床试验注册编号:NCT00099242。