Scordo Michael, Bhatt Valkal, Hsu Meier, Omuro Antonio M, Matasar Matthew J, DeAngelis Lisa M, Dahi Parastoo B, Moskowitz Craig H, Giralt Sergio A, Sauter Craig S
Department of Medicine, Adult Bone Marrow Transplant Service, Memorial Sloan Kettering Cancer Center, New York, New York.
Department of Medicine, Adult Bone Marrow Transplant Service, Memorial Sloan Kettering Cancer Center, New York, New York.
Biol Blood Marrow Transplant. 2017 Jan;23(1):38-43. doi: 10.1016/j.bbmt.2016.09.024. Epub 2016 Oct 3.
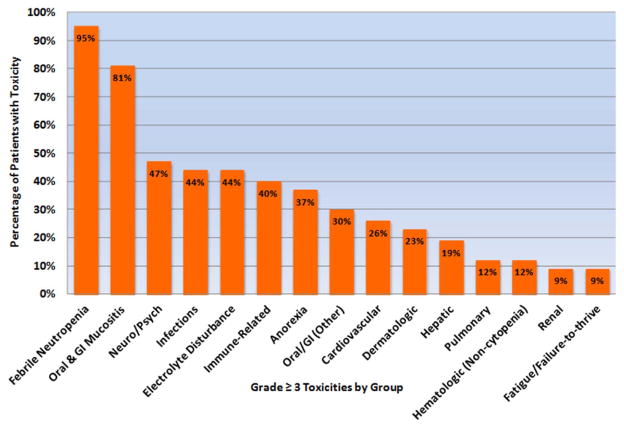
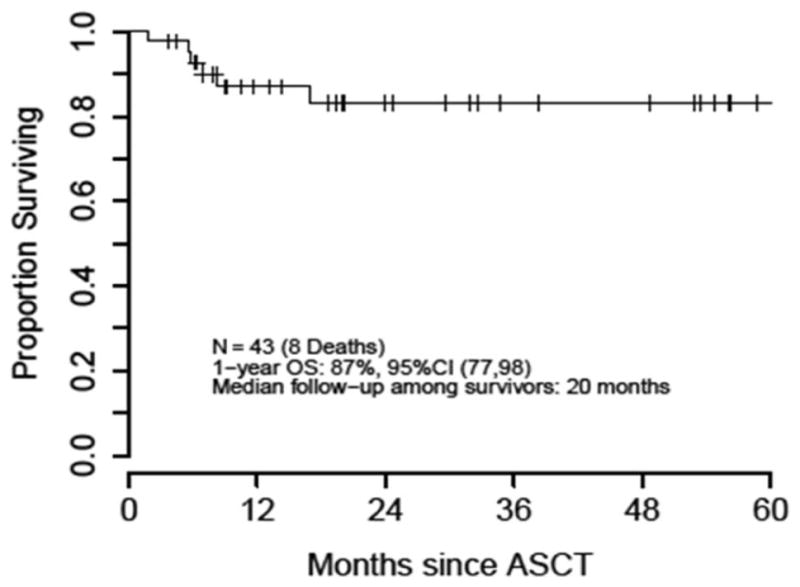
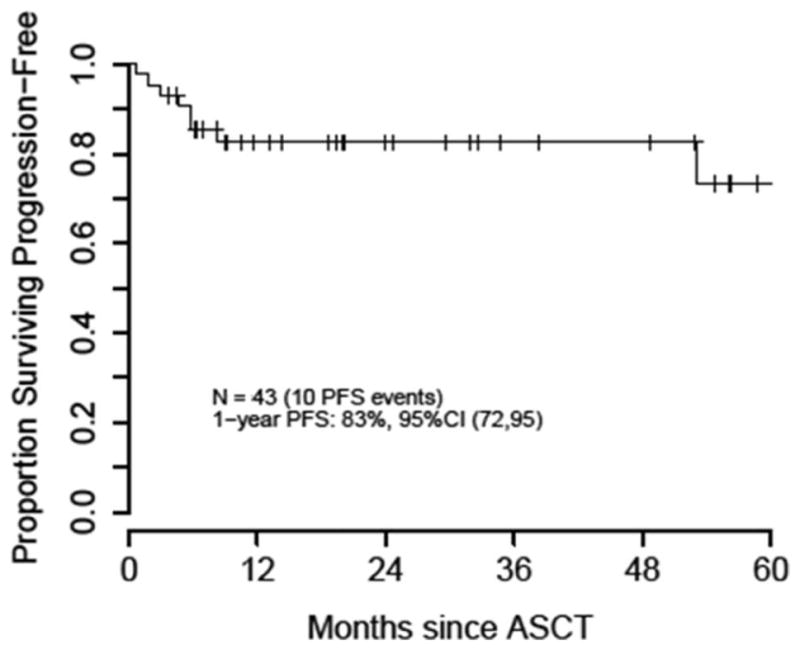
High-dose therapy and autologous stem cell transplantation (ASCT) with thiotepa, busulfan, and cyclophosphamide (TBC) conditioning has emerged as an effective postinduction treatment strategy for patients with primary central nervous system lymphoma (PCNSL) or secondary central nervous system lymphoma (SCNSL), but it is associated with considerable toxicity and transplantation-related mortality (TRM) in the modern era. Forty-three adult patients with chemosensitive PCNSL or SCNSL underwent TBC-conditioned ASCT between 2006 and 2015. Twenty-eight of these patients received pharmacokinetically (PK)-targeted busulfan dosing. The median number of clinically relevant individual grade ≥3 nonhematologic toxicities per patient was 5. We found no association between pretransplantation patient characteristics and the presence of more than 5 grade ≥3 nonhematologic toxicities. Patients with elevated first-dose busulfan area under the curve values did not experience more toxicity. Paradoxically, patients treated with more than 2 regimens before undergoing ASCT had lower first-dose busulfan AUC values. With a median follow-up among survivors of 20 months, 1-year progression-free survival (PFS) and overall survival (OS) from the time of ASCT were 83% and 87%, respectively. Although this study reaffirms the favorable PFS and OS associated with TBC-conditioned ASCT for PCNSL or SCNSL, this treatment strategy carries a large toxicity burden.
采用噻替派、白消安和环磷酰胺(TBC)预处理的大剂量疗法及自体干细胞移植(ASCT)已成为原发性中枢神经系统淋巴瘤(PCNSL)或继发性中枢神经系统淋巴瘤(SCNSL)患者诱导缓解后的一种有效治疗策略,但在现代,它与相当大的毒性及移植相关死亡率(TRM)相关。2006年至2015年间,43例对化疗敏感的PCNSL或SCNSL成年患者接受了TBC预处理的ASCT。其中28例患者接受了基于药代动力学(PK)的白消安剂量调整。每位患者临床上相关的≥3级非血液学毒性的中位数为5次。我们发现移植前患者特征与≥5次≥3级非血液学毒性的存在之间无关联。首次剂量白消安曲线下面积值升高的患者并未出现更多毒性。矛盾的是,在接受ASCT前接受超过2种方案治疗的患者首次剂量白消安的AUC值较低。在幸存者中,中位随访20个月,自ASCT时起1年无进展生存期(PFS)和总生存期(OS)分别为83%和87%。尽管本研究再次证实了TBC预处理的ASCT对PCNSL或SCNSL具有良好的PFS和OS,但这种治疗策略具有很大的毒性负担。