Moon Jangsup, Kim Do-Yong, Byun Jung-Ick, Sunwoo Jun-Sang, Lim Jung-Ah, Kim Tae-Joon, Shin Jung-Won, Lee Woo-Jin, Lee Han Sang, Jun Jin-Sun, Park Kyung-Il, Jung Keun-Hwa, Lee Soon-Tae, Jung Ki-Young, Chu Kon, Lee Sang Kun
Department of Neurology, Laboratory for Neurotherapeutics, Comprehensive Epilepsy Center, Center for Medical Innovations, Biomedical Research Institute, Seoul National University Hospital, Seoul, Republic of Korea.
Program in Neuroscience, Seoul National University College of Medicine, Seoul, Republic of Korea.
Health Qual Life Outcomes. 2016 Oct 12;14(1):144. doi: 10.1186/s12955-016-0548-x.
Patients with postural tachycardia syndrome often appear depressive and report diminished quality of life (QOL). In the current study, we first evaluated if the maximal heart rate (HR) increment after standing is associated with the clinical symptoms in patients with excessive orthostatic tachycardia (OT). Next, we investigated the correlations among the symptoms of orthostatic intolerance (OI), depression, and health-related QOL in these patients. Finally we assessed if patients with minimal OI symptoms suffer from depression or diminished QOL.
We performed a comprehensive questionnaire-based assessment of symptoms in 107 patients with excessive OT with a ≥ 30 beats/min heart rate increment (or ≥ 40 beats/min in individuals aged between 12 and 19) within 10 min after standing up. An existing orthostatic intolerance questionnaire (OIQ), the Beck depression inventory-II (BDI-II), and the 36 Item Short-Form Health Survey were completed prior to any treatment. Correlation analyses among the items of the questionnaires and other parameters were performed. Additionally, patients with minimal OI symptoms were analysed separately.
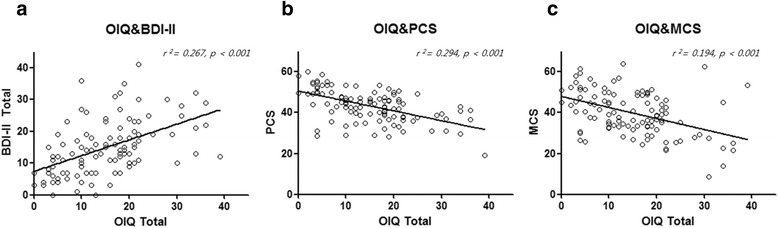
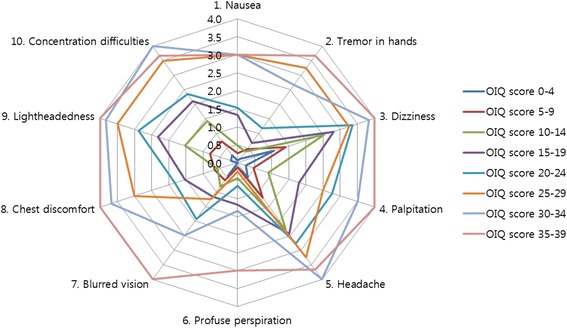
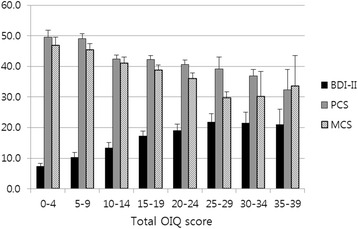
The maximal orthostatic HR increment was not associated with the clinical symptoms. The OI symptoms were significantly correlated with depression and diminished QOL. The BDI-II score demonstrated a positive linear relationship with total OIQ score (r = 0.516), and both physical and mental component summary scales of SF-36 showed a negative linear relationship with total OIQ score (r = -0.542 and r = -0.440, respectively; all p <0.001). Some OI symptoms were more strongly associated with depression, and others were more strongly related to QOL. Chest discomfort and concentration difficulties were the most influential OI symptoms for depression, while nausea and concentration difficulties were the most influential symptoms for physical and mental QOL, respectively. Dizziness and headache were the two most common complaints in patients with mild to moderate OI symptoms. In addition, subjects with minimal OI symptoms also had considerable deterioration in QOL.
The OI symptoms, but not the maximal HR increment, are significantly correlated with depression and diminished QOL in patients with excessive OT. Therefore, pervasive history taking is important when encountering patients with excessive OT.
体位性心动过速综合征患者常出现抑郁情绪,并报告生活质量(QOL)下降。在本研究中,我们首先评估站立后最大心率(HR)增量是否与直立性心动过速(OT)过度患者的临床症状相关。接下来,我们调查了这些患者体位性不耐受(OI)症状、抑郁与健康相关生活质量之间的相关性。最后,我们评估了OI症状轻微的患者是否患有抑郁症或生活质量下降。
我们对107例OT过度患者进行了基于问卷的全面症状评估,这些患者在站立后10分钟内心率增量≥30次/分钟(12至19岁个体心率增量≥40次/分钟)。在进行任何治疗之前,完成了现有的体位性不耐受问卷(OIQ)、贝克抑郁量表第二版(BDI-II)和36项简短健康调查。对问卷项目与其他参数进行了相关性分析。此外,对OI症状轻微的患者进行了单独分析。
最大直立性HR增量与临床症状无关。OI症状与抑郁和生活质量下降显著相关。BDI-II评分与OIQ总评分呈正线性关系(r = 0.516),SF-36的身体和心理成分汇总量表与OIQ总评分均呈负线性关系(分别为r = -0.542和r = -0.440;所有p < 0.001)。一些OI症状与抑郁的关联更强,而另一些则与生活质量的关联更强。胸部不适和注意力不集中是对抑郁影响最大的OI症状,而恶心和注意力不集中分别是对身体和心理生活质量影响最大的症状。头晕和头痛是轻度至中度OI症状患者最常见的两种主诉。此外,OI症状轻微的受试者生活质量也有相当程度的下降。
在OT过度的患者中,OI症状而非最大HR增量与抑郁和生活质量下降显著相关。因此,在遇到OT过度的患者时,全面的病史采集很重要。