Itakura Jun, Kurosaki Masayuki, Hasebe Chitomi, Osaki Yukio, Joko Kouji, Yagisawa Hitoshi, Sakita Shinya, Okushin Hiroaki, Satou Takashi, Hisai Hiroyuki, Abe Takehiko, Tsuji Keiji, Tamada Takashi, Kobashi Haruhiko, Mitsuda Akeri, Ide Yasushi, Ogawa Chikara, Tsuruta Syotaro, Takaguchi Kouichi, Murakawa Miyako, Asahina Yasuhiro, Enomoto Nobuyuki, Izumi Namiki
Department of Gastroenterology and Hepatology, Musashino Red Cross Hospital, Musashino, Tokyo, Japan.
Department of Gastroenterology, Japanese Red Cross Asahikawa Hospital, Asahikawa, Hokkaido, Japan.
PLoS One. 2016 Oct 24;11(10):e0165339. doi: 10.1371/journal.pone.0165339. eCollection 2016.
BACKGROUNDS & AIMS: We aimed to clarify the characteristics of resistance-associated substitutions (RASs) after treatment failure with NS5A inhibitor, daclatasvir (DCV) in combination with NS3/4A inhibitor, asunaprevir (ASV), in patients with chronic hepatitis C virus genotype 1b infection.
This is a nationwide multicenter study conducted by the Japanese Red Cross Liver Study Group. The sera were obtained from 68 patients with virological failure after 24 weeks of DCV/ASV treatment. RASs in NS5A and NS3 were determined by population sequencing.
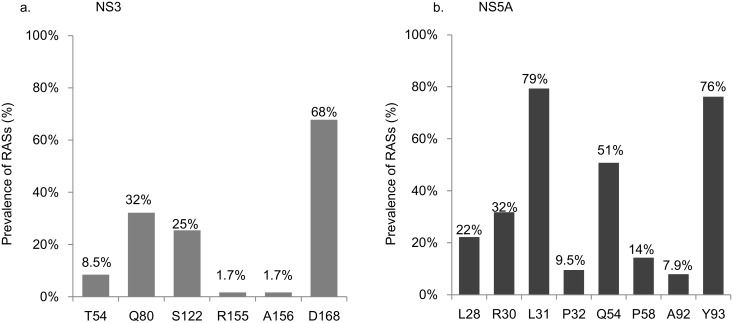
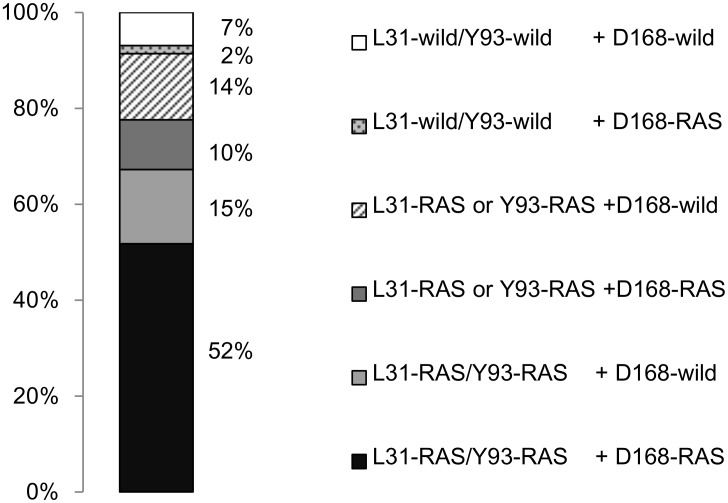
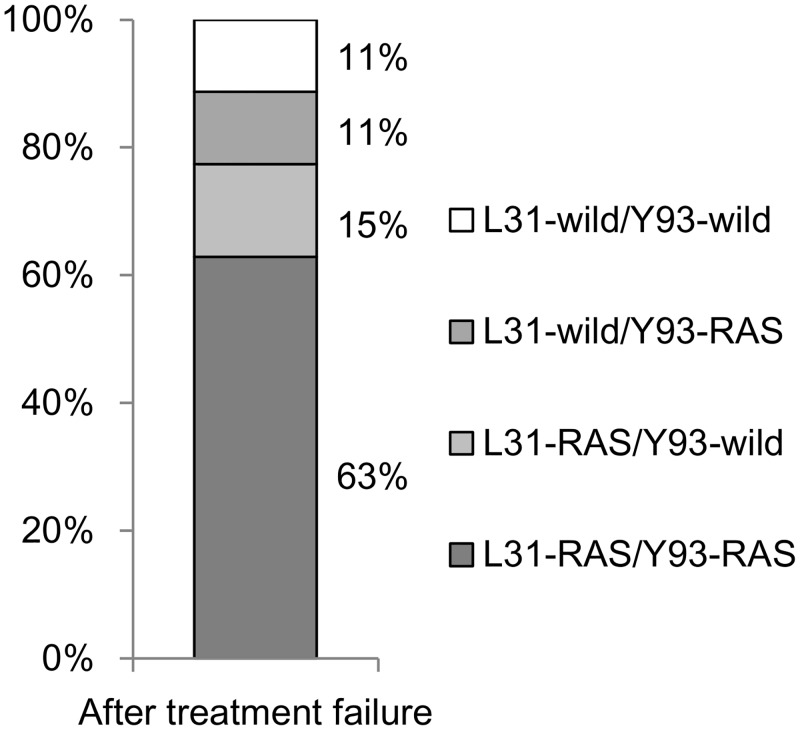
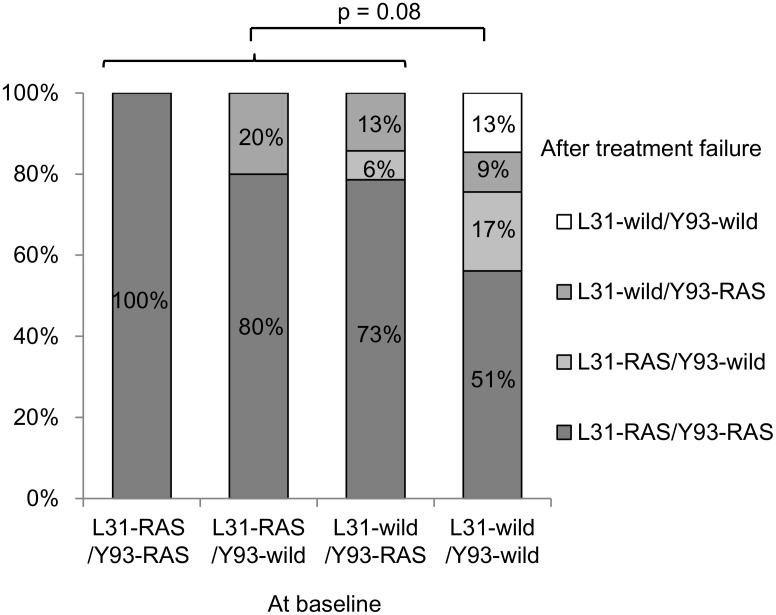
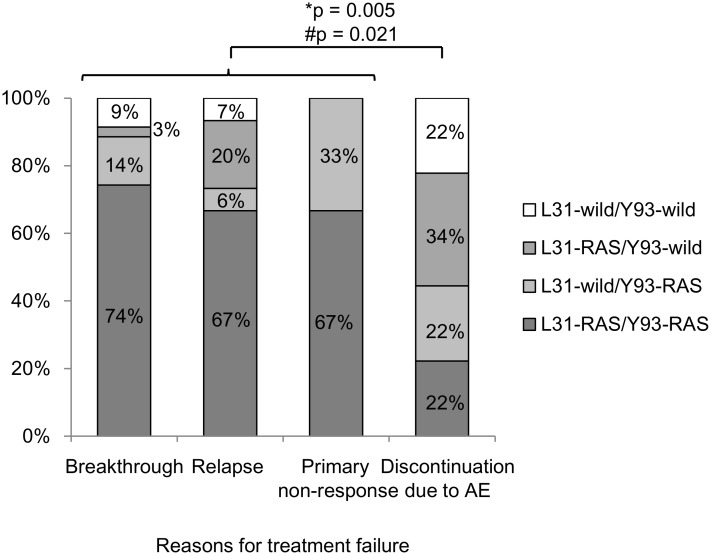
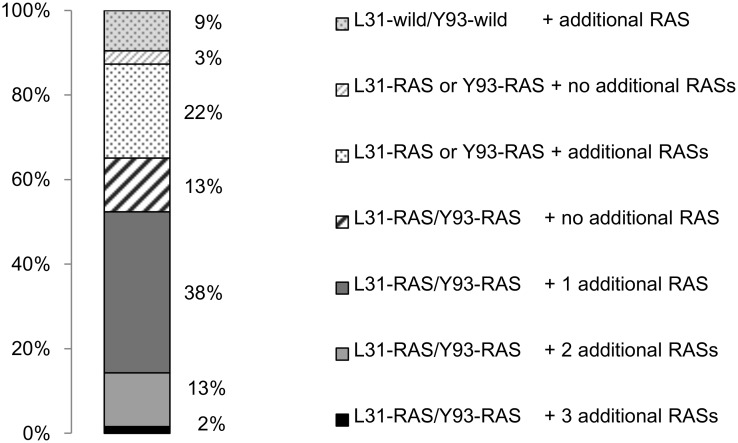
The frequency of signature RASs at position D168 of NS3 was 68%, and at positions L31 and Y93 of NS5A was 79 and 76%, respectively. The frequency of dual signature RASs in NS5A (L31-RAS and Y93-RAS) was 63%. RASs at L28, R30, P32, Q54, P58, and A92 in addition to dual signature RAS were detected in 5, 5, 1, 22, 2, and 0 patients, respectively. In total, triple, quadruple, and quintuple RASs in combination with dual signature RAS were detected in 35, 10, and 1.5% patients, respectively. These RASs were detected in patients without baseline RASs or who prematurely discontinued therapy. Co-existence of D168 RAS in NS3 and L31 and/or Y93 RAS in NS5A was observed in 62% of patients.
Treatment-emergent RASs after failure with DCV/ASV combination therapy are highly complex in more than 50% of the patients. The identification of complex RAS patterns, which may indicate high levels of resistance to NS5A inhibitors, highlights the need for RAS sequencing when considering re-treatment with regimens including NS5A inhibitors.
我们旨在阐明在慢性丙型肝炎病毒1b型感染患者中,使用NS5A抑制剂达卡他韦(DCV)联合NS3/4A抑制剂阿舒瑞韦(ASV)治疗失败后,耐药相关替代位点(RASs)的特征。
这是一项由日本红十字会肝脏研究组开展的全国多中心研究。血清取自68例接受DCV/ASV治疗24周后出现病毒学失败的患者。通过群体测序确定NS5A和NS3中的RASs。
NS3的D168位点特征性RASs的频率为68%,NS5A的L31和Y93位点的频率分别为79%和76%。NS5A中双重特征性RASs(L31-RAS和Y93-RAS)的频率为63%。除双重特征性RAS外,L28、R30、P32、Q54、P58和A92位点的RASs分别在5、5、1、22、2和0例患者中检测到。总共分别在35%、10%和1.5%的患者中检测到与双重特征性RAS联合存在的三重、四重和五重RASs。这些RASs在无基线RASs或过早停药的患者中检测到。62%的患者中观察到NS3的D168 RAS与NS5A的L31和/或Y93 RAS共存。
超过50%的患者在DCV/ASV联合治疗失败后出现的治疗中出现的RASs高度复杂。复杂RAS模式的识别可能表明对NS5A抑制剂的高耐药水平,这突出了在考虑使用含NS5A抑制剂的方案重新治疗时进行RAS测序的必要性。