Loudin Michael, Anderson Sharon, Schlansky Barry
Department of Medicine, Division of Gastroenterology & Hepatology, Oregon Health & Science University, 3181 SW Sam Jackson Park Road, Portland, OR, L-461, USA.
Department of Medicine, Division of Nephrology, Oregon Health & Science University, 3181 SW Sam Jackson Park Road, Portland, OR, USA.
BMC Gastroenterol. 2016 Oct 24;16(1):134. doi: 10.1186/s12876-016-0548-7.
Proximal or 'downhill' esophageal varices are a rare cause of upper gastrointestinal hemorrhage. Unlike the much more common distal esophageal varices, which are most commonly a result of portal hypertension, downhill esophageal varices result from vascular obstruction of the superior vena cava (SVC). While SVC obstruction is most commonly secondary to malignant causes, our review of the literature suggests that benign causes of SVC obstruction are the most common cause actual bleeding from downhill varices. Given the alternative pathophysiology of downhill varices, they require a unique approach to management. Variceal band ligation may be used to temporize acute variceal bleeding, and should be applied on the proximal end of the varix. Relief of the underlying SVC obstruction is the cornerstone of definitive treatment of downhill varices.
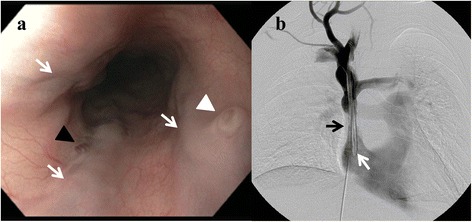
A young woman with a benign superior vena cava stenosis due to a tunneled internal jugular vein dialysis catheter presented with hematemesis and melena. Urgent upper endoscopy revealed multiple 'downhill' esophageal varices with stigmata of recent hemorrhage. As there was no active bleeding, no endoscopic intervention was performed. CT angiography demonstrated stenosis of the SVC surrounding the distal tip of her indwelling hemodialysis catheter. The patient underwent balloon angioplasty of the stenotic SVC segment with resolution of her bleeding and clinical stabilization.
Downhill esophageal varices are a distinct entity from the more common distal esophageal varices. Endoscopic therapies have a role in temporizing active variceal bleeding, but relief of the underlying SVC obstruction is the cornerstone of treatment and should be pursued as rapidly as possible. It is unknown why benign, as opposed to malignant, causes of SVC obstruction result in bleeding from downhill varices at such a high rate, despite being a less common etiology of SVC obstruction.
近端或“下行性”食管静脉曲张是上消化道出血的罕见原因。与更常见的远端食管静脉曲张不同,后者最常见的原因是门静脉高压,而下行性食管静脉曲张是由上腔静脉(SVC)血管阻塞引起的。虽然SVC阻塞最常见于恶性病因,但我们对文献的回顾表明,SVC阻塞的良性病因是下行性静脉曲张实际出血的最常见原因。鉴于下行性静脉曲张的病理生理学不同,它们需要独特的管理方法。曲张静脉套扎术可用于暂时控制急性曲张静脉出血,应在曲张静脉的近端进行。缓解潜在的SVC阻塞是下行性静脉曲张确定性治疗的基石。
一名年轻女性因隧道式颈内静脉透析导管导致良性上腔静脉狭窄,出现呕血和黑便。紧急上消化道内镜检查发现多处“下行性”食管静脉曲张并有近期出血迹象。由于没有活动性出血,未进行内镜干预。CT血管造影显示其留置血液透析导管远端周围的SVC狭窄。患者接受了狭窄SVC段的球囊血管成形术,出血得到缓解,临床症状稳定。
下行性食管静脉曲张与更常见的远端食管静脉曲张是不同的实体。内镜治疗在暂时控制活动性曲张静脉出血方面有作用,但缓解潜在的SVC阻塞是治疗的基石,应尽快进行。尚不清楚为什么与恶性病因相反,SVC阻塞的良性病因会导致下行性静脉曲张如此高比例的出血,尽管它是SVC阻塞的较不常见病因。