Sudulagunta Sreenivasa Rao, Sepehrar Mona, Sodalagunta Mahesh Babu, Settikere Nataraju Aravinda, Bangalore Raja Shiva Kumar, Sathyanarayana Deepak, Gummadi Siddharth, Burra Hemanth Kumar
Columbia Asia Hospital, Kirloskar Business Park, Hebbal, Bangalore, India.
Baptist Hospital, Bangalore, India.
Ger Med Sci. 2016 Oct 13;14:Doc12. doi: 10.3205/000239. eCollection 2016.
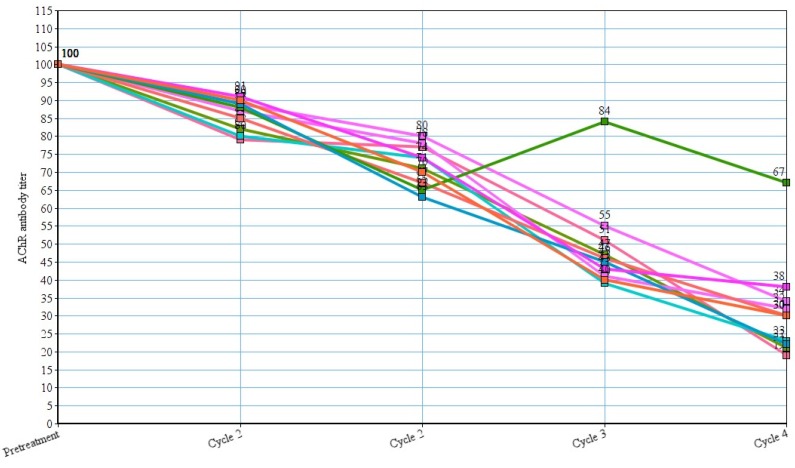
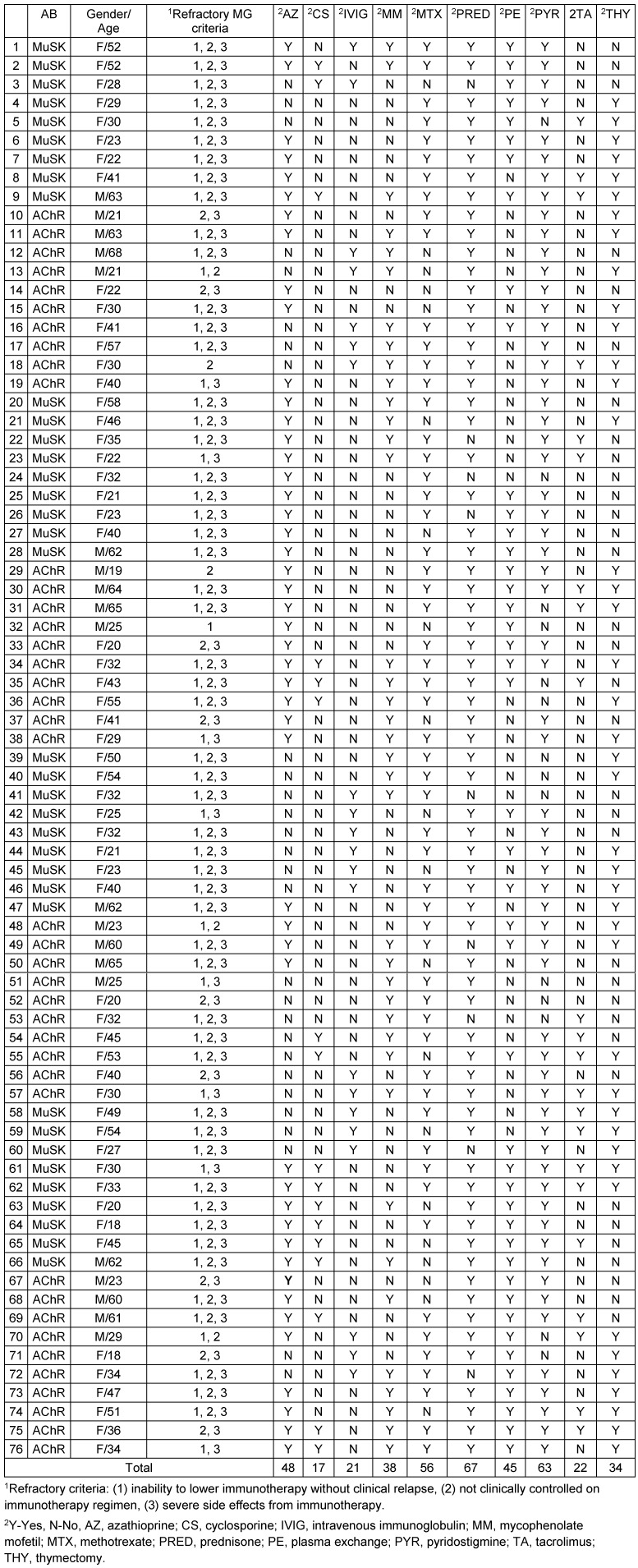
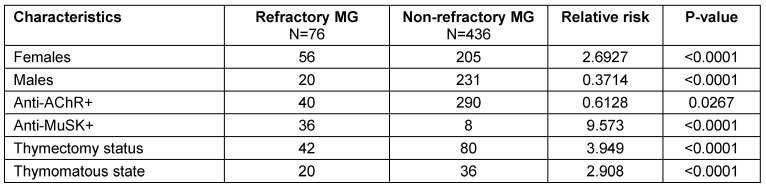
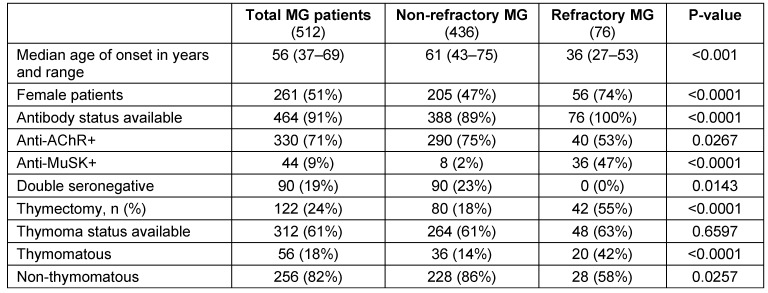
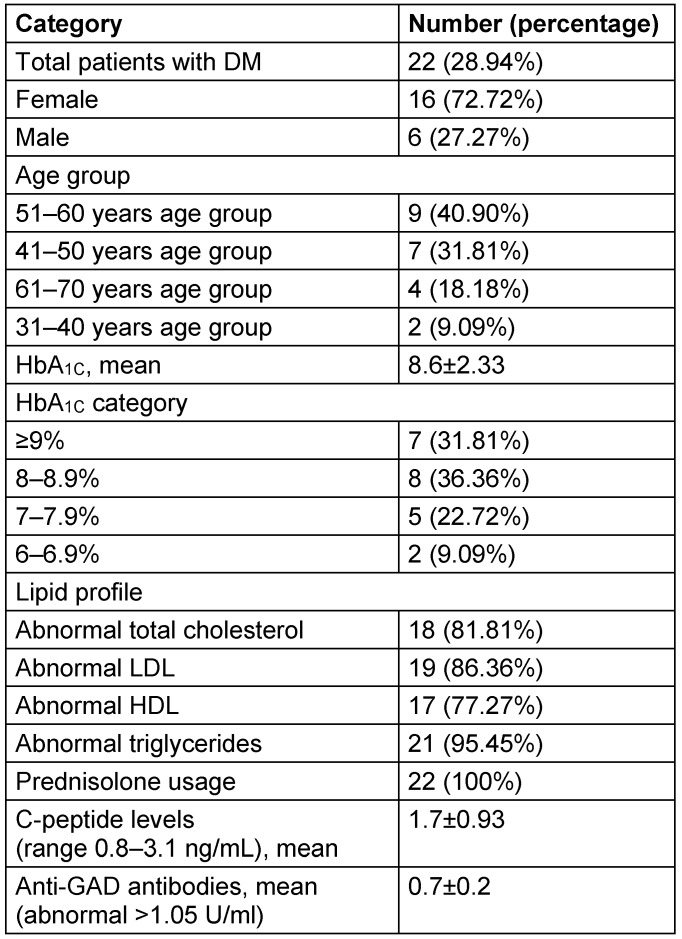
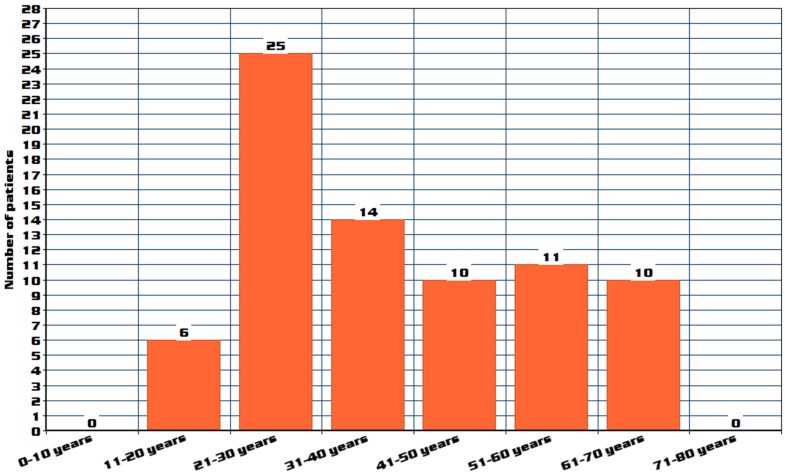
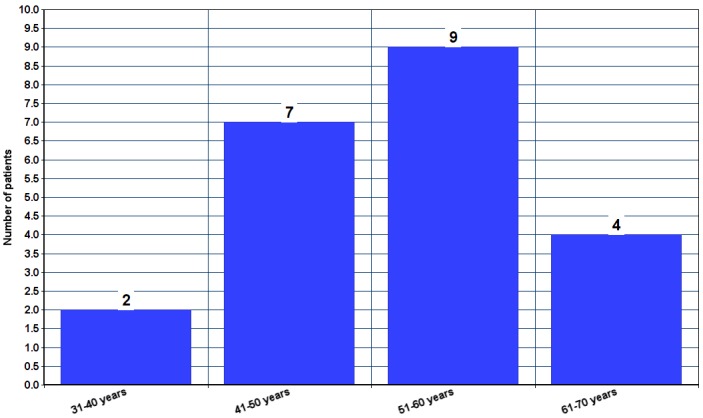
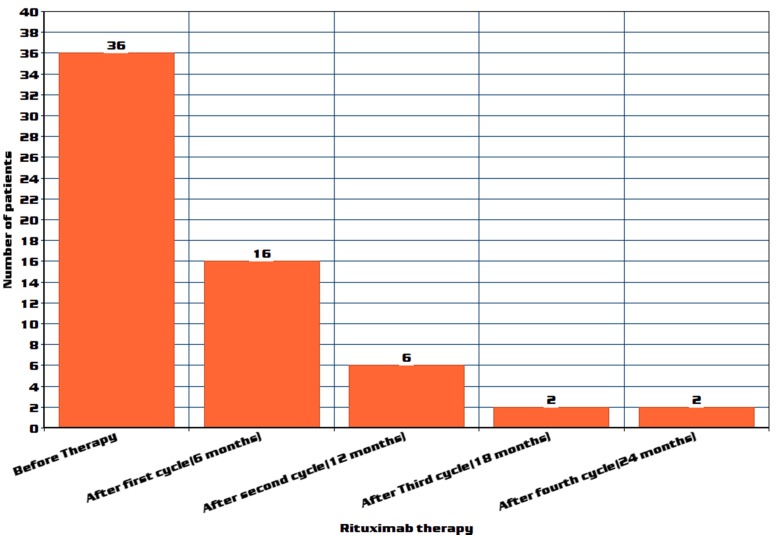
Myasthenia gravis (MG) is an antibody mediated autoimmune neuromuscular disorder characterized by fatigable muscle weakness. A proportion of myasthenia gravis patients are classified as refractory due to non responsiveness to conventional treatment. This retrospective study was done to evaluate clinical profile, epidemiological, laboratory, and features of patients with MG and mode of management using rituximab and complications. Data of myasthenia gravis patients admitted or presented to outpatient department (previous medical records) with MG between January 2008 and January 2016 were included. A total of 512 patients fulfilled the clinical and diagnostic criteria of myasthenia gravis of which 76 patients met the diagnostic certainty for refractory myasthenia gravis and were evaluated. Out of 76 refractory MG patients, 53 (69.73%) patients fulfilled all the three defined criteria. The median age of onset of the refractory MG group was 36 years with a range of 27-53 years. In our study 25 patients (32.89%) belonged to the age group of 21-30 years. Anti-MuSK antibodies were positive in 8 non-refractory MG patients (2.06%) and 36 refractory MG patients (47.36%). Mean HbA was found to be 8.6±2.33. The dose of administered prednisone decreased by a mean of 59.7% (=3.3x10) to 94.6% (=2.2x10) after the third cycle of rituximab treatment. The refractory MG patients are most commonly female with an early age of onset, anti-MuSK antibodies, and thymomas. Refractory MG patients have higher prevalence and poor control (HbA >8%) of diabetes mellitus and dyslipidemia probably due to increased steroid usage. Rituximab is very efficient in treatment of refractory MG with adverse effects being low.
重症肌无力(MG)是一种由抗体介导的自身免疫性神经肌肉疾病,其特征为易疲劳性肌肉无力。一部分重症肌无力患者因对传统治疗无反应而被归类为难治性患者。本回顾性研究旨在评估重症肌无力患者的临床特征、流行病学、实验室检查结果以及使用利妥昔单抗的治疗方式和并发症。纳入了2008年1月至2016年1月期间因重症肌无力入住或就诊于门诊(既往病历)的患者数据。共有512例患者符合重症肌无力的临床和诊断标准,其中76例符合难治性重症肌无力的诊断确定性并接受了评估。在76例难治性重症肌无力患者中,53例(69.73%)满足所有三项既定标准。难治性重症肌无力组的发病年龄中位数为36岁,范围为27至53岁。在我们的研究中,25例患者(32.89%)属于21至30岁年龄组。8例非难治性重症肌无力患者(2.06%)和36例难治性重症肌无力患者(47.36%)的抗MuSK抗体呈阳性。平均糖化血红蛋白(HbA)为8.6±2.33。在利妥昔单抗治疗的第三个周期后,泼尼松的给药剂量平均降低了59.7%(=3.3x10)至94.6%(=2.2x10)。难治性重症肌无力患者最常见于女性,发病年龄较早,存在抗MuSK抗体和胸腺瘤。难治性重症肌无力患者糖尿病和血脂异常的患病率较高且控制不佳(HbA>8%),可能是由于类固醇使用增加所致。利妥昔单抗在治疗难治性重症肌无力方面非常有效,不良反应较少。