Massoullié Grégoire, Bordachar Pierre, Irles Didier, Caussin Christophe, Da Costa Antoine, Defaye Pascal, Jean Frédéric, Mechulan Alexis, Mondoly Pierre, Souteyrand Géraud, Pereira Bruno, Ploux Sylvain, Eschalier Romain
Clermont Université, Université d'Auvergne, Cardio Vascular Interventional Therapy and Imaging (CaVITI), Image Science for Interventional Techniques (ISIT), UMR6284, Clermont-Ferrand, France.
Cardiology Department, CHU Clermont-Ferrand, Clermont-Ferrand, France.
BMJ Open. 2016 Oct 26;6(10):e010485. doi: 10.1136/bmjopen-2015-010485.
Percutaneous aortic valve replacement (transcatheter aortic valve implantation (TAVI)) notably increases the likelihood of the appearance of a complete left bundle branch block (LBBB) by direct lesion of the LBB of His. This block can lead to high-grade atrioventricular conduction disturbances responsible for a poorer prognosis. The management of this complication remains controversial.
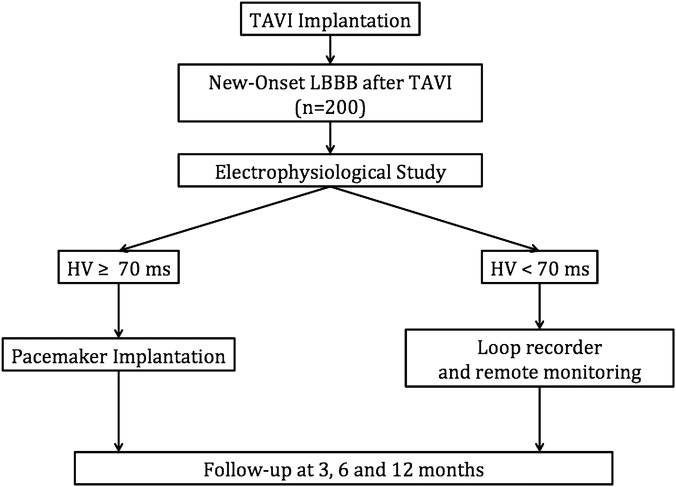
The screening of LBBB after TAVI persisting for more than 24 hours will be conducted by surface ECG. Stratification will be performed by post-TAVI intracardiac electrophysiological study. Patients at high risk of conduction disturbances (≥70 ms His-ventricle interval (HV) or presence of infra-Hisian block) will be implanted with a pacemaker enabling the recording of disturbance episodes. Those at lower risk (HV <70 ms) will be implanted with a loop recorder device with remote monitoring of cardiovascular implantable electronic devices (CIEDs). Clinical, ECG and implanted device follow-up will also be performed at 3, 6 and 12 months. The primary objective is to assess the efficacy and safety of a decisional algorithm based on electrophysiological study and remote monitoring of CIEDs in the prediction of high-grade conduction disturbances in patients with LBBB after TAVI. The primary end point is to compare the incidence (rate and time to onset) of high-grade conduction disturbances in patients with LBBB after TAVI between the two groups at 12 months. Given the proportion of high-grade conduction disturbances (20-40%), a sample of 200 subjects will allow a margin of error of 6-7%. The LBBB-TAVI Study has been in an active recruiting phase since September 2015 (21 patients already included).
Local ethics committee authorisation was obtained in May 2015. We will publish findings from this study in a peer-reviewed scientific journal and present results at national and international conferences.
NCT02482844; Pre-results.
经皮主动脉瓣置换术(经导管主动脉瓣植入术(TAVI))显著增加了因希氏束左束支直接损伤而出现完全性左束支传导阻滞(LBBB)的可能性。这种阻滞可导致高度房室传导障碍,预后较差。该并发症的处理仍存在争议。
通过体表心电图对TAVI术后持续超过24小时的LBBB进行筛查。将通过TAVI术后的心内电生理研究进行分层。传导障碍高危患者(希氏束-心室间期(HV)≥70毫秒或存在希氏束下阻滞)将植入能够记录障碍发作的起搏器。低危患者(HV<70毫秒)将植入具有心血管植入式电子设备(CIED)远程监测功能的环形记录仪。还将在3、6和12个月时进行临床、心电图和植入设备随访。主要目的是评估基于电生理研究和CIED远程监测的决策算法在预测TAVI术后LBBB患者高度传导障碍方面的有效性和安全性。主要终点是比较两组在12个月时TAVI术后LBBB患者高度传导障碍的发生率(发生率和发作时间)。鉴于高度传导障碍的比例(20%-40%),200名受试者的样本将允许6%-7%的误差范围。自2015年9月以来,LBBB-TAVI研究一直处于积极招募阶段(已纳入21名患者)。
2015年5月获得当地伦理委员会批准。我们将在同行评审的科学期刊上发表本研究的结果,并在国内和国际会议上展示结果。
NCT0,248,2844;预结果。