Bais Babette, Kamperman Astrid M, van der Zwaag Marjolein D, Dieleman Gwen C, Harmsen van der Vliet-Torij Hanneke W, Bijma Hilmar H, Lieverse Ritsaert, Hoogendijk Witte J G, Lambregtse-van den Berg Mijke P
Department of Psychiatry, Erasmus University Medical Centre Rotterdam, 's Gravendijkwal 230, 3015CE, Rotterdam, The Netherlands.
Epidemiological and Social Psychiatric Research Institute, Erasmus University Medical Centre Rotterdam, 's Gravendijkwal 230, 3015 CE, Rotterdam, The Netherlands.
BMC Psychiatry. 2016 Nov 8;16(1):381. doi: 10.1186/s12888-016-1092-2.
Depression during pregnancy is a common and high impact disease. Generally, 5-10 % of pregnant women suffer from depression. Children who have been exposed to maternal depression during pregnancy have a higher risk of adverse birth outcomes and more often show cognitive, emotional and behavioural problems. Therefore, early detection and treatment of antepartum depression is necessary. Both psychotherapy and antidepressant medication, first choice treatments in a non-pregnant population, have limitations in treating depression during pregnancy. Therefore, it is urgent and relevant to investigate alternative treatments for antepartum depression. Bright light therapy (BLT) is a promising treatment for pregnant women with depressive disorder, for it combines direct availability, sufficient efficacy, low costs and high safety, taking the safety for the unborn child into account as well.
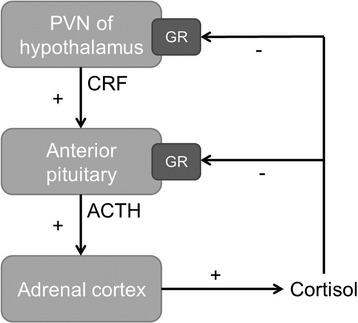
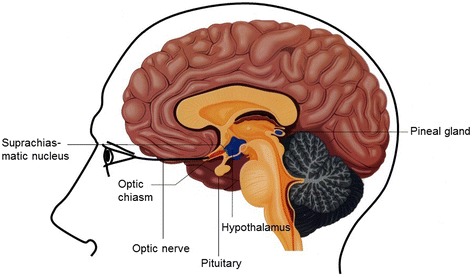
In this study, 150 pregnant women (12-18 weeks pregnant) with a DSM-V diagnosis of depressive disorder will be randomly allocated in a 1:1 ratio to one of the two treatment arms: treatment with BLT (9.000 lux) or treatment with dim red light therapy (100 lux). Both groups will be treated for 6 weeks at home on a daily basis for 30 min, within 30 min of habitual wake-up time. Follow-up will take place after 6 weeks of therapy, 3 and 10 weeks after end of therapy, at birth and 2, 6 and 18 months postpartum. Primary outcome will be the average change in depressive symptoms between the two groups, as measured by the Structured Interview Guide for the Hamilton Depression Scale - Seasonal Affective Disorder version and the Edinburg Postnatal Depression Scale. Changes in rating scale scores of these questionnaires over time will be analysed using generalized linear mixed models. Secondary outcomes will be the changes in maternal cortisol and melatonin levels, in maternal sleep quality and gestational age, birth weight, infant behaviour, infant cortisol exposure and infant cortisol stress response.
If BLT reduces depressive symptoms in pregnant women, it will provide a safe, cheap, non-pharmacological and efficacious alternative treatment for psychotherapy and antidepressant medication in treating antepartum depression, without any expected adverse reactions for the unborn child.
Netherlands Trial Register NTR5476 . Registered 5 November 2015.
孕期抑郁症是一种常见且影响较大的疾病。一般来说,5%至10%的孕妇患有抑郁症。孕期暴露于母亲抑郁症的儿童出现不良出生结局的风险更高,且更常表现出认知、情感和行为问题。因此,产前抑郁症的早期检测和治疗很有必要。心理治疗和抗抑郁药物是未怀孕人群的首选治疗方法,但在治疗孕期抑郁症方面都有局限性。因此,研究产前抑郁症的替代治疗方法迫在眉睫且具有现实意义。强光疗法(BLT)是治疗患有抑郁症的孕妇的一种有前景的治疗方法,因为它兼具直接可用性、足够的疗效、低成本和高安全性,同时也考虑到了对未出生胎儿的安全性。
在本研究中,150名孕周为12至18周且被诊断为DSM-V抑郁症的孕妇将按1:1的比例随机分配到两个治疗组之一:接受强光疗法(9000勒克斯)治疗或接受暗红色光疗法(100勒克斯)治疗。两组均在家中每天治疗30分钟,在习惯起床时间的30分钟内进行,为期6周。治疗6周后、治疗结束后3周和10周、分娩时以及产后2个月、6个月和18个月进行随访。主要结局将是两组之间抑郁症状的平均变化,通过汉密尔顿抑郁量表 - 季节性情感障碍版结构化访谈指南和爱丁堡产后抑郁量表进行测量。这些问卷评分量表分数随时间的变化将使用广义线性混合模型进行分析。次要结局将是母亲皮质醇和褪黑素水平的变化、母亲睡眠质量、孕周、出生体重、婴儿行为、婴儿皮质醇暴露和婴儿皮质醇应激反应的变化。
如果强光疗法能减轻孕妇的抑郁症状,它将为心理治疗和抗抑郁药物治疗产前抑郁症提供一种安全、廉价、非药物且有效的替代治疗方法,且对未出生胎儿无任何预期的不良反应。
荷兰试验注册NTR5476。2015年11月5日注册。