Hurnakova Jana, Hulejova Hana, Zavada Jakub, Komarc Martin, Hanova Petra, Klein Martin, Mann Herman, Sleglova Olga, Olejarova Marta, Forejtova Sarka, Ruzickova Olga, Vencovsky Jiri, Pavelka Karel, Senolt Ladislav
Institute of Rheumatology, Prague, Czech Republic.
Rheumatology Department, First Faculty of Medicine, Charles University, Prague, Czech Republic.
PLoS One. 2016 Nov 10;11(11):e0165498. doi: 10.1371/journal.pone.0165498. eCollection 2016.
Clinical remission in some patients with rheumatoid arthritis (RA) may be associated with ongoing synovial inflammation that is not always detectable on clinical examination or reflected by laboratory tests but can be visualized by musculoskeletal ultrasound. The goal of our study was to determine the levels of serum calprotectin, a major leukocyte protein, in patients with RA in clinical remission and to investigate the ability of serum calprotectin levels to distinguish patients in ultrasound-defined remission from those with residual ultrasound subclinical inflammation.
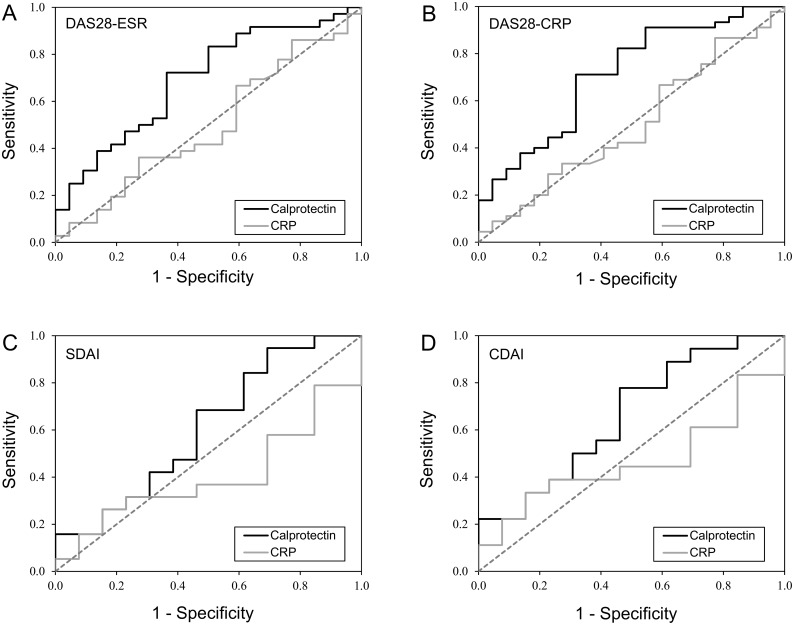
Seventy RA patients in clinical remission underwent clinical and ultrasound examination. Ultrasound examination was performed according to the German US7 score. Ultrasound remission was defined as grey scale (GS) range 0-1 and power Doppler (PD) range 0. The levels of serum calprotectin and C-reactive protein (CRP) were determined. The discriminatory capacity of calprotectin and CRP in detecting residual ultrasound inflammation was assessed using ROC curves.
The total number of patients fulfilling the DAS28-ESR, DAS28-CRP, SDAI and CDAI remission criteria was 58, 67, 32 and 31, respectively. Residual synovial inflammation was found in 58-67% of the patients who fulfilled at least one set of clinical remission criteria. Calprotectin levels were significantly higher in patients with residual synovial inflammation than in those with ultrasound-defined remission (mean 2.5±1.3 vs. 1.7±0.8 μg/mL, p<0.005). Using ultrasound-defined remission criteria, calprotectin had an AUC of 0.692, p<0.05 using DAS28-ESR remission criteria and an AUC of 0.712, p<0.005 using DAS28-CRP remission criteria. Calprotectin correctly distinguished ultrasound remission from subclinical activity in 70% of patients. CRP (AUC DAS28-ESR = 0.494, p = NS; AUC DAS28-CRP = 0.498, p = NS) had lower and insignificant discriminatory capacity.
The present study demonstrates the potential of calprotectin to distinguish RA patients in both clinical and ultrasound-defined remission from patients in clinical remission but with residual subclinical disease activity.
部分类风湿关节炎(RA)患者的临床缓解可能与持续存在的滑膜炎症相关,这种炎症在临床检查中并不总是能被检测到,也未通过实验室检查反映出来,但可通过肌肉骨骼超声显示。我们研究的目的是确定临床缓解的RA患者血清钙卫蛋白(一种主要的白细胞蛋白)水平,并研究血清钙卫蛋白水平区分超声定义的缓解患者与有残余超声亚临床炎症患者的能力。
70例临床缓解的RA患者接受临床和超声检查。超声检查按照德国US7评分进行。超声缓解定义为灰阶(GS)范围0 - 1且能量多普勒(PD)范围0。测定血清钙卫蛋白和C反应蛋白(CRP)水平。使用ROC曲线评估钙卫蛋白和CRP检测残余超声炎症的鉴别能力。
符合DAS28 - ESR、DAS28 - CRP、SDAI和CDAI缓解标准的患者总数分别为58、67、32和31例。在至少符合一组临床缓解标准的患者中,58% - 67%存在残余滑膜炎症。有残余滑膜炎症的患者钙卫蛋白水平显著高于超声定义缓解的患者(均值2.5±1.3 vs. 1.7±0.8 μg/mL,p<0.005)。使用超声定义的缓解标准,钙卫蛋白的AUC为0.692,使用DAS28 - ESR缓解标准时p<0.05,使用DAS28 - CRP缓解标准时AUC为0.712,p<0.005。钙卫蛋白在70%的患者中正确区分了超声缓解与亚临床活动。CRP(AUC DAS28 - ESR = 0.494,p = 无显著性差异;AUC DAS28 - CRP = 0.498,p = 无显著性差异)的鉴别能力较低且无显著性差异。
本研究证明了钙卫蛋白区分临床缓解以及超声定义缓解的RA患者与临床缓解但有残余亚临床疾病活动患者的潜力。