Kobayashi Takashi, Kubota Masayuki, Arai Yuhki, Ohyama Toshiyuki, Yokota Naoki, Miura Kohei, Ishikawa Hirosuke, Soma Daiki, Takizawa Kazuyasu, Sakata Jun, Nagahashi Masayuki, Kameyama Hitoshi, Wakai Toshifumi
Department of Pediatric Surgery, Niigata University Graduate School of Medical and Dental Sciences, 1-757, Asahimachi-dori, Chu-o-ku, Niigata, 951-8510, Japan.
Division of Digestive and General Surgery, Niigata University Graduate School of Medical and Dental Sciences, Niigata, Japan.
Surg Case Rep. 2016 Dec;2(1):134. doi: 10.1186/s40792-016-0264-0. Epub 2016 Nov 16.
Severe blunt hepatic injury is a major cause of morbidity and mortality in pediatric patients. Damage control (DC) surgery has been reported to be useful in severely compromised children with hepatic injury. We applied such a technique in the treatment of a case of hemodynamically unstable grade IV blunt hepatic injury in an eight-year-old girl. This case is the first to use multimodal approaches including perihepatic packing, temporary closure of the abdominal wall with a plastic sheet, transarterial embolization (TAE), and planned delayed anatomical hepatic resection in a child.
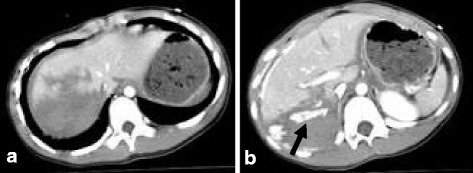
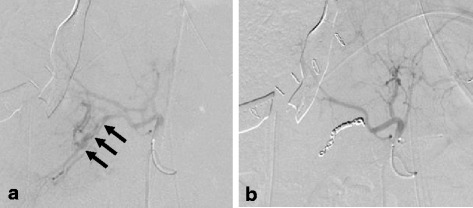
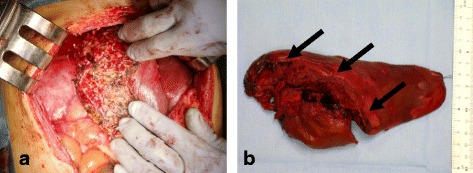
An eight-year-old girl was run over by a motor vehicle and transferred to the emergency department of the local hospital. Her diagnoses were severe blunt hepatic injury (grade IV) with left femoral trochanteric fracture. No other organ injuries were observed. Because her hemodynamic state was stable under aggressive fluid resuscitation, she was transferred to our hospital for surgical management. On arrival at our institution about 4 h after the injury, her hemodynamic condition became unstable. Abdominal compartment syndrome also became apparent. Because her condition had deteriorated and the lethal triad of low BT, coagulopathy, and acidosis was observed, a DC treatment strategy was selected. First, emergent laparotomy was performed for gauze-packing hemostasis to control intractable bleeding from the liver bed, and the abdomen was temporarily closed with a plastic sheet with continuous negative pressure aspiration. Transarterial embolization of the posterior branch of the right hepatic artery was then carried out immediately after the operation. The lacerated right lobe of the liver was safely resected in a stable hemodynamic condition 2 days after the initial operation. Bleeding from the liver bed ceased without further need of hemostasis. She was transferred to the local hospital without any surgical complications on day 42 after admission. She had returned to her normal life by 3 months after the injury.
The DC strategy was found to be effective even in a pediatric patient with hemodynamically unstable severe blunt hepatic injury. The presence of the deadly triad (hypothermia, coagulopathy, and acidosis) and abdominal compartment syndrome was an indication for DC surgery.
严重钝性肝损伤是儿科患者发病和死亡的主要原因。据报道,损伤控制(DC)手术对严重肝损伤的儿童患者有用。我们将这种技术应用于一名8岁女孩的血流动力学不稳定的IV级钝性肝损伤的治疗。该病例是首例在儿童中使用包括肝周填塞、用塑料片临时关闭腹壁、经动脉栓塞(TAE)以及计划性延迟解剖性肝切除术在内的多模式方法。
一名8岁女孩被机动车碾压后被送往当地医院急诊科。她的诊断为严重钝性肝损伤(IV级)伴左股骨转子骨折。未观察到其他器官损伤。由于在积极液体复苏下她的血流动力学状态稳定,她被转至我院进行手术治疗。受伤后约4小时到达我院时,她的血流动力学状况变得不稳定。腹腔间隔室综合征也很明显。由于她的病情恶化且观察到低体温、凝血功能障碍和酸中毒这一致命三联征,选择了DC治疗策略。首先,进行急诊剖腹手术,用纱布填塞止血以控制来自肝床的顽固性出血,并用带有持续负压吸引的塑料片临时关闭腹部。术后立即对右肝动脉后支进行经动脉栓塞。在初次手术后2天,在血流动力学稳定的情况下安全切除了肝脏右叶的裂伤部分。肝床出血停止,无需进一步止血。入院后第42天,她被转至当地医院,无任何手术并发症。受伤后3个月她已恢复正常生活。
发现DC策略即使在血流动力学不稳定的严重钝性肝损伤的儿科患者中也有效。致命三联征(低体温、凝血功能障碍和酸中毒)和腹腔间隔室综合征的存在是DC手术的指征。