Burkhalter F, Schaub S, Bucher Ch, Gürke L, Bachmann A, Hopfer H, Dickenmann M, Steiger J, Binet I
Clinic for Transplant Immunology and Nephrology, University Hospital Basel, Basel, Switzerland.
Nephrology and Transplantation Medicine, Kantonsspital St Gallen, St Gallen, Switzerland.
PLoS One. 2016 Nov 17;11(11):e0165233. doi: 10.1371/journal.pone.0165233. eCollection 2016.
Induction treatment with rabbit polyclonal antithymocyte globulins (ATGs) is frequent used in kidney transplant recipients with donorspecific HLA antibodies and shows acceptable outcomes. The two commonly used ATGs, Thymoglobulin and ATG-F have slightly different antigen profile and antibody concentrations. The two compounds have never been directly compared in a prospective trial in immunological high-risk recipients. Therefore we performed a prospective randomized controlled study comparing the two compounds in immunological high-risk kidney recipients in terms of safety and efficacy.
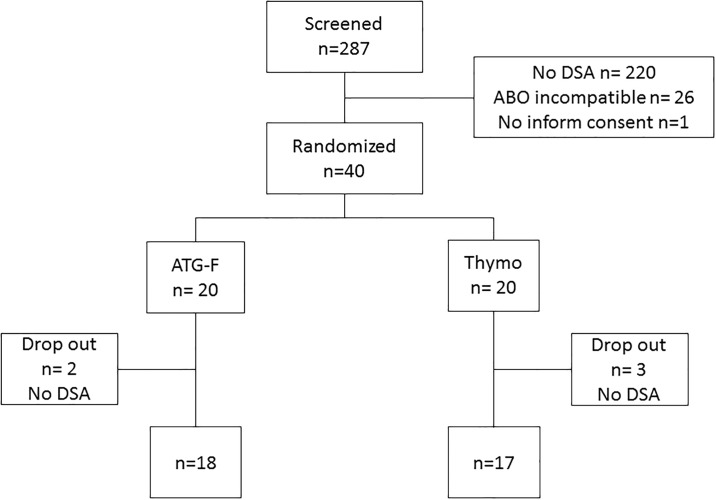
Immunological high-risk kidney recipients, defined as the presence of HLA DSA but negative CDC-B and T-cell crossmatches were randomized 1:1 to receive ATG-F or Thymoglobulin. Maintenance immunosuppressive therapy consisted of tacrolimus, mycophenolate mofetil and steroids.
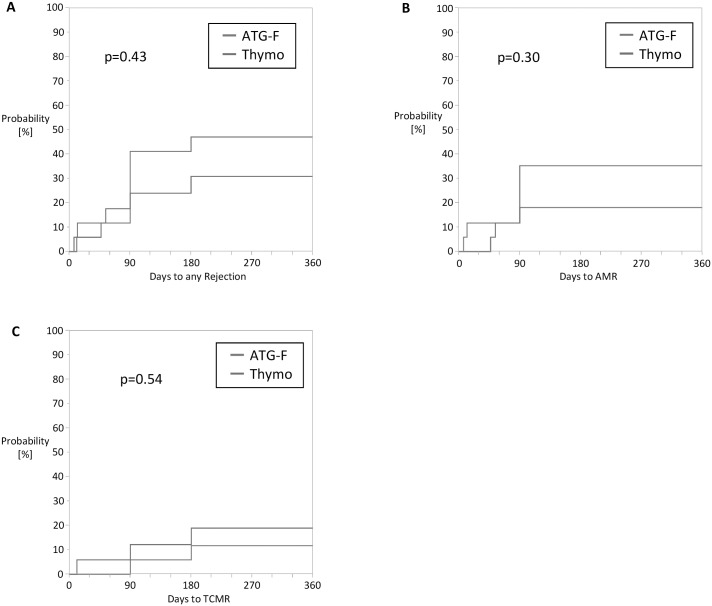
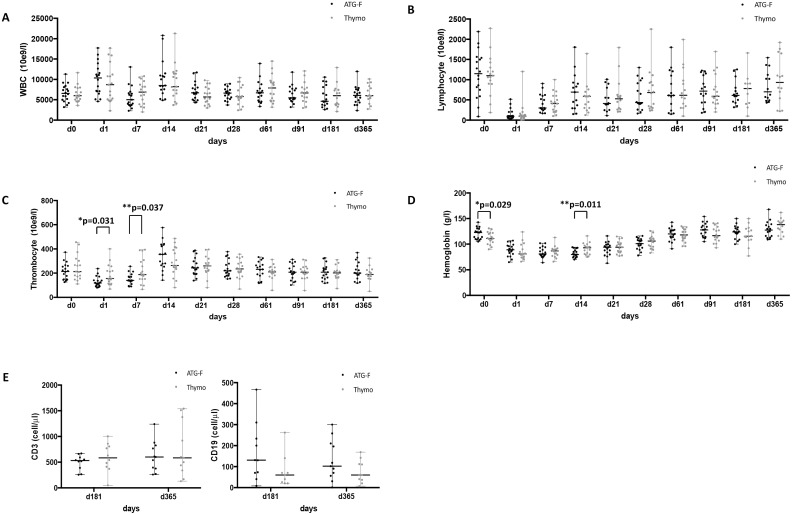
The per-protocol analysis included 35 patients. There was no immediate infusion reaction observed with both compounds. No PTLD or malignancy occurred during the follow-up in both groups. The incidence of viral and bacterial infections was similar in both groups (p = 0.62). The cumulative incidence of clinical and subclinical antibody mediated allograft rejection as well as T-cell mediated allograft rejection during the first year between ATG-F and Thymoglobulin was similar (35% versus 19%; p = 0.30 and 11% versus 18%; 0.54 respectively). The two-year graft function was similar with a median eGFR of 56 ml/min/1.73m2 (range 21-128) (ATG-F-group) and 51 ml/min/1.73m2 (range 22-132) (Thymo-group) (p = 0.69).
We found no significant differences between the compared study drugs for induction treatment in immunological high-risk patients regarding safety and efficacy during follow-up with good allograft function at 2 years after transplantation.
兔多克隆抗胸腺细胞球蛋白(ATG)诱导治疗常用于有供体特异性HLA抗体的肾移植受者,且疗效尚可。两种常用的ATG,即胸腺球蛋白和ATG - F,其抗原谱和抗体浓度略有不同。这两种化合物从未在免疫高风险受者的前瞻性试验中进行过直接比较。因此,我们进行了一项前瞻性随机对照研究,比较这两种化合物在免疫高风险肾移植受者中的安全性和有效性。
将免疫高风险肾移植受者(定义为存在HLA DSA但CDC - B和T细胞交叉配型阴性)按1:1随机分组,分别接受ATG - F或胸腺球蛋白治疗。维持免疫抑制治疗包括他克莫司、霉酚酸酯和类固醇。
符合方案分析纳入了35例患者。两种化合物均未观察到即刻输注反应。两组随访期间均未发生PTLD或恶性肿瘤。两组病毒和细菌感染的发生率相似(p = 0.62)。ATG - F组和胸腺球蛋白组在第一年临床和亚临床抗体介导的移植肾排斥反应以及T细胞介导的移植肾排斥反应的累积发生率相似(分别为35%对19%;p = 0.30和11%对18%;0.54)。两年的移植肾功能相似,ATG - F组的平均肾小球滤过率(eGFR)中位数为56 ml/min/1.73m²(范围21 - 128),胸腺球蛋白组为51 ml/min/1.73m²(范围22 - 132)(p = 0.69)。
我们发现,在免疫高风险患者诱导治疗中,所比较的研究药物在随访期间的安全性和有效性方面无显著差异,移植后2年移植肾功能良好。