Kiiski K, Lehtokari V-L, Manzur A Y, Sewry C, Zaharieva I, Muntoni F, Pelin K, Wallgren-Pettersson C
The Folkhälsan Institute of Genetics and the Department of Medical and Clinical Genetics, Medicum, University of Helsinki, Helsinki, Finland.
Great Ormond Street Hospital, London, UK.
J Neuromuscul Dis. 2015 Sep 21;2(4):433-438. doi: 10.3233/JND-150107.
Nemaline myopathy may be caused by pathogenic variants in the TPM3 gene and is then called NEM1. All previously identified disease-causing variants are point mutations including missense, nonsense and splice-site variants. The aim of the study was to identify the disease-causing gene in this patient and verify the NM diagnosis.
Mutation analysis methods include our self-designed nemaline myopathy array, The Nemaline Myopathy Comparative Genomic Hybridisation Array (NM-CGH array), whole-genome array-CGH, dHPLC, Sanger sequencing and whole-exome sequencing. The diagnostic muscle biopsy was investigated further by routine histopathological methods.
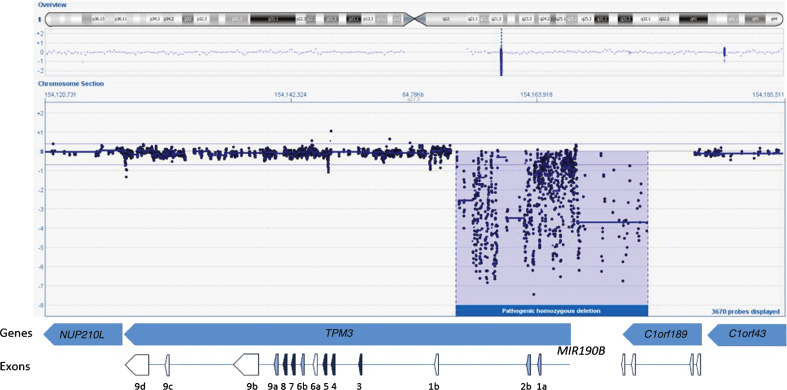
We present here the first large (17-21 kb) aberration in the α-tropomyosinslow gene (TPM3), identified using the NM-CGH array. This homozygous deletion removes the exons 1a and 2b as well as the promoter of the TPM3 isoform encoding Tpm3.12st. The severe phenotype included paucity of movement, proximal and axial weakness and feeding difficulties requiring nasogastric tube feeding. The infant died at the age of 17.5 months. Muscle biopsy showed variation in fibre size and rods in a population of hypotrophic muscle fibres expressing slow myosin, often with internal nuclei, and abnormal immunolabelling revealing many hybrid fibres.
This is the only copy number variation we have identified in any NM gene other than nebulin (NEB), suggesting that large deletions or duplications in these genes are very rare, yet possible, causes of NM.
杆状体肌病可能由TPM3基因的致病变异引起,这种情况下被称为NEM1。此前所有已鉴定出的致病变体均为点突变,包括错义突变、无义突变和剪接位点变体。本研究的目的是鉴定该患者的致病基因并验证杆状体肌病的诊断。
突变分析方法包括我们自行设计的杆状体肌病基因芯片、杆状体肌病比较基因组杂交芯片(NM - CGH芯片)、全基因组芯片 - CGH、变性高效液相色谱(dHPLC)、桑格测序和全外显子组测序。通过常规组织病理学方法对诊断性肌肉活检样本进行进一步研究。
我们在此展示了使用NM - CGH芯片鉴定出的首例α - 原肌球蛋白慢基因(TPM3)中的大片段(17 - 21 kb)畸变。这种纯合缺失去除了外显子1a和2b以及编码Tpm3.12st的TPM3异构体的启动子。严重的表型包括活动减少、近端和躯干肌无力以及需要鼻饲管喂养的喂养困难。该婴儿在17.5个月时死亡。肌肉活检显示,在一群表达慢肌球蛋白的萎缩性肌纤维中,纤维大小存在差异且有杆状体,这些肌纤维常含有内部细胞核,异常免疫标记显示有许多杂种纤维。
这是我们在除伴肌动蛋白(NEB)之外的任何杆状体肌病基因中鉴定出的唯一拷贝数变异,表明这些基因中的大片段缺失或重复是非常罕见但有可能的杆状体肌病病因。