Crusoe Edvan de Queiroz, Higashi Fabiana, Martinez Gracia Aparecida, Barros José Carlos, Bellesso Marcelo, Rossato Marina, Marret Ana Cinira F, Chiattone Carlos Sérgio, Hungria Vania Tietsch de Moraes
Faculdade de Ciências Médicas da Santa Casa de São Paulo (FCMSCSP), São Paulo, SP, Brazil.
Faculdade de Ciências Médicas da Santa Casa de São Paulo (FCMSCSP), São Paulo, SP, Brazil.
Rev Bras Hematol Hemoter. 2016 Oct-Dec;38(4):302-309. doi: 10.1016/j.bjhh.2016.06.004. Epub 2016 Jul 29.
Cyclophosphamide plus thalidomide as induction for multiple myeloma patients eligible for autologous stem cell transplantation may be a limiting factor for cell mobilization. The minimum acceptable mobilized peripheral blood stem cell count to prevent deleterious effects during transplantation is 2.0×10 CD34 cells/kg. Combining other treatments to granulocyte-colony stimulating factor, such as cyclophosphamide, could overcome the mobilization limitation. The objective of this study was to assess the number of CD34 cells mobilized using granulocyte-colony stimulating factor with and without cyclophosphamide after induction with cyclophosphamide, thalidomide and dexamethasone.
A retrospective study was performed of a cohort of multiple myeloma patients submitted to autologous stem cell transplantations at two Brazilian centers between May 2009 and July 2013. The oral cyclophosphamide and thalidomide induction doses used were 1500mg/month and 100-200mg/day, respectively. Mobilization doses were 10-15mcg/kg granulocyte-colony stimulating factor with 2-4g/m cyclophosphamide, or 15-20mcg/kg granulocyte-colony stimulating factor alone for 5 days. Collection of >2.0×10 CD34 cells/kg was considered sufficient.
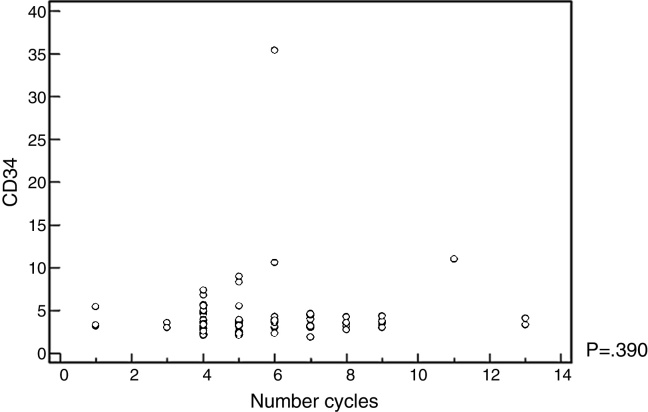
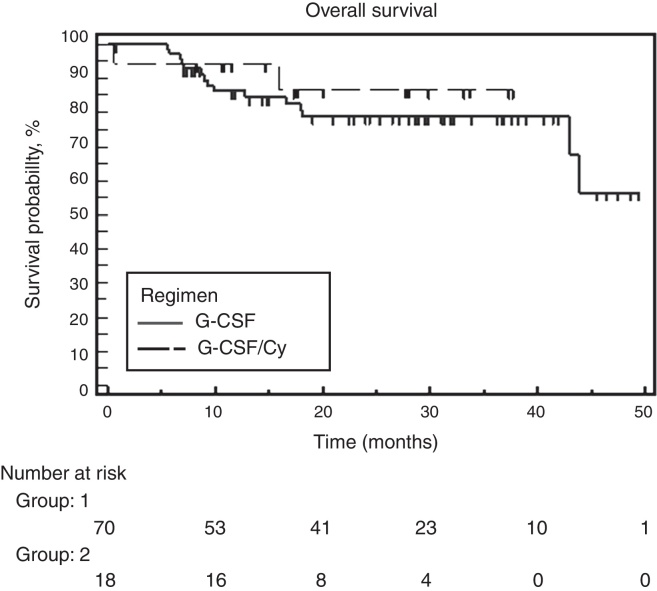
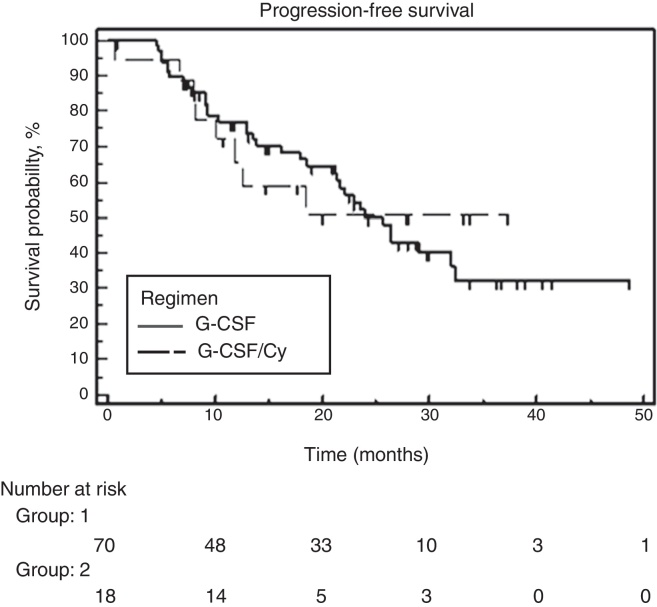
Eighty-eight patients were analyzed; only 18 received cyclophosphamide. The median age was 58 years old (range: 51-62) for the granulocyte-colony stimulating factor group and 56.5 years old (range: 54-60) for granulocyte-colony stimulating factor plus cyclophosphamide group. Fifty-two patients were male. Eighty cases (90.9%) were Durie-Salmon Staging System III-A/B and 38 (44.7%) and 20 cases (23.5%) were International Staging System 2 and 3, respectively. The group that received cyclophosphamide collected a higher median number of progenitor cells [3.8 (range: 3.1-4.4) vs. 3.2 (range: 2.3-3.8)] (p-value=0.008). No correlation was observed between better responses or number of induction cycles and the number of cells collected.
The number of cells mobilized with granulocyte-colony stimulating factor plus cyclophosphamide was higher. However, in both groups, the median number of CD34 cells was sufficient to perform a single autologous stem cell transplantation; no deleterious effects were reported during harvesting.
环磷酰胺联合沙利度胺用于适合自体干细胞移植的多发性骨髓瘤患者诱导治疗时,可能是细胞动员的一个限制因素。预防移植期间产生有害影响的可接受的最低动员外周血干细胞计数为2.0×10 CD34细胞/kg。将其他治疗与粒细胞集落刺激因子联合使用,如环磷酰胺,可克服动员限制。本研究的目的是评估在使用环磷酰胺、沙利度胺和地塞米松诱导后,使用粒细胞集落刺激因子联合或不联合环磷酰胺动员的CD34细胞数量。
对2009年5月至2013年7月间在巴西两个中心接受自体干细胞移植的一组多发性骨髓瘤患者进行回顾性研究。口服环磷酰胺和沙利度胺的诱导剂量分别为1500mg/月和100 - 200mg/天。动员剂量为10 - 15mcg/kg粒细胞集落刺激因子联合2 - 4g/m环磷酰胺,或单独使用15 - 20mcg/kg粒细胞集落刺激因子,持续5天。收集到>2.0×10 CD34细胞/kg被认为是足够的。
分析了88例患者;仅18例接受了环磷酰胺治疗。粒细胞集落刺激因子组的中位年龄为58岁(范围:51 - 62岁),粒细胞集落刺激因子联合环磷酰胺组为56.5岁(范围:54 - 60岁)。52例患者为男性。80例(90.9%)为Durie - Salmon分期系统III - A/B期,国际分期系统2期和期分别为38例(44.7%)和20例(23.5%)。接受环磷酰胺治疗的组收集的祖细胞中位数更高[3.8(范围:3.1 - 4.4)对3.2(范围:2.3 - 3.8)](p值 = 0.008)。未观察到较好反应或诱导周期数与收集的细胞数之间存在相关性。
粒细胞集落刺激因子联合环磷酰胺动员的细胞数量更高。然而,在两组中,CD34细胞中位数足以进行单次自体干细胞移植;采集过程中未报告有害影响。