Reproductive Medicine Centre, Skane University Hospital, Malmö, Sweden.
Department of Oncology, Skane University Hospital, Malmö, Sweden.
Asian J Androl. 2017 Sep-Oct;19(5):538-542. doi: 10.4103/1008-682X.191126.
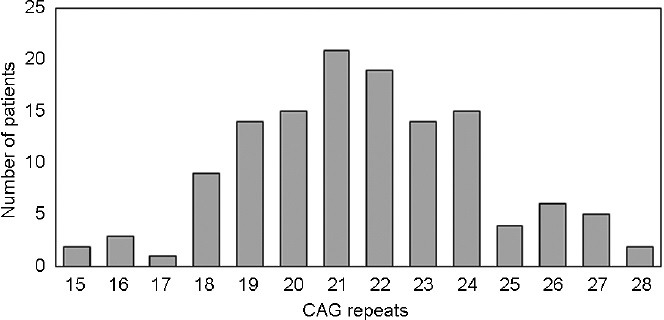
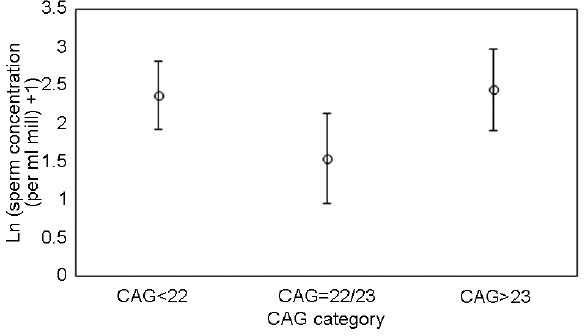
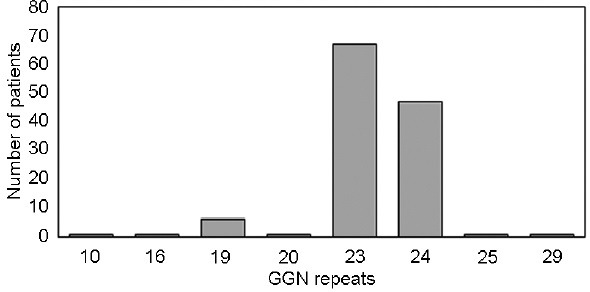
Spermatogenesis is an androgen-regulated process that depends on the action of androgen receptor (AR). Sperm production may be affected in men treated for testicular cancer (TC), and it is important to identify the factors influencing the timing of spermatogenesis recovery following cancer treatment. It is known that the CAG and GGN repeat numbers affect the activity of the AR; therefore, the aim of this study is to investigate if the CAG and GGN polymorphisms in the AR gene predict recovery of sperm production after TC treatment. TC patients (n = 130) delivered ejaculates at the following time points: postorchiectomy and at 6, 12, 24, 36, and 60 months posttherapy (T0, T6, T12, T24, T36, and T60). The CAG lengths were categorized into three groups, <22 CAG, 22-23 CAG, and >23 CAG, and the GGN tracts were also categorized into three groups, <23 GGN, 23 GGN, and >23 GGN. At T12, men with 22-23 CAG presented with a statistically significantly (P = 0.045) lower sperm concentration than those with other CAG numbers (8.4 × 106 ml-1 vs 16 × 106 ml-1 ; 95% CI: 1.01-2.65). This association was robust to omitting adjustment for treatment type and sperm concentration at T0 (P = 0.021; 3.7 × 106 ml-1 vs 10 × 106 ml-1 ; 95% CI: 1.13-4.90). The same trends were observed for total sperm number. The least active AR variant seems to be associated with a more rapid recovery of spermatogenesis. This finding adds to our understanding of the biology of postcancer therapy recovery of fertility in males and has clinical implications.
精子发生是一个雄激素调节的过程,依赖于雄激素受体(AR)的作用。接受睾丸癌(TC)治疗的男性的精子生成可能会受到影响,因此确定影响癌症治疗后精子发生恢复时间的因素非常重要。已知 CAG 和 GGN 重复数会影响 AR 的活性;因此,本研究旨在探讨 AR 基因中的 CAG 和 GGN 多态性是否可预测 TC 治疗后精子生成的恢复情况。TC 患者(n = 130)在以下时间点射出精液:睾丸切除术和治疗后 6、12、24、36 和 60 个月(T0、T6、T12、T24、T36 和 T60)。CAG 长度分为三组,<22 CAG、22-23 CAG 和 >23 CAG,GGN 片段也分为三组,<23 GGN、23 GGN 和 >23 GGN。在 T12 时,22-23 CAG 的男性精子浓度明显低于其他 CAG 数(8.4×106ml-1 与 16×106ml-1;95%CI:1.01-2.65)(P = 0.045)。这种关联在排除治疗类型和 T0 时精子浓度的调整后仍然稳健(P = 0.021;3.7×106ml-1 与 10×106ml-1;95%CI:1.13-4.90)。总精子数也呈现出相同的趋势。最不活跃的 AR 变体似乎与更快的精子发生恢复有关。这一发现增加了我们对男性癌症治疗后生育能力恢复生物学的理解,具有临床意义。