Lozeron Pierre, Poujois Aurélia, Richard Alexandra, Masmoudi Sana, Meppiel Elodie, Woimant France, Kubis Nathalie
Service de Physiologie Clinique-Explorations Fonctionnelles, AP-HP, Hôpital LariboisièreParis, France; INSERM UMR965Paris, France; Sorbonne Paris Cité - Université Paris DiderotParis, France.
Service de Neurologie, AP-HP, Hôpital LariboisièreParis, France; Centre de Référence National de la Maladie de Wilson, Hôpital LariboisièreParis, France.
Front Neural Circuits. 2016 Nov 10;10:90. doi: 10.3389/fncir.2016.00090. eCollection 2016.
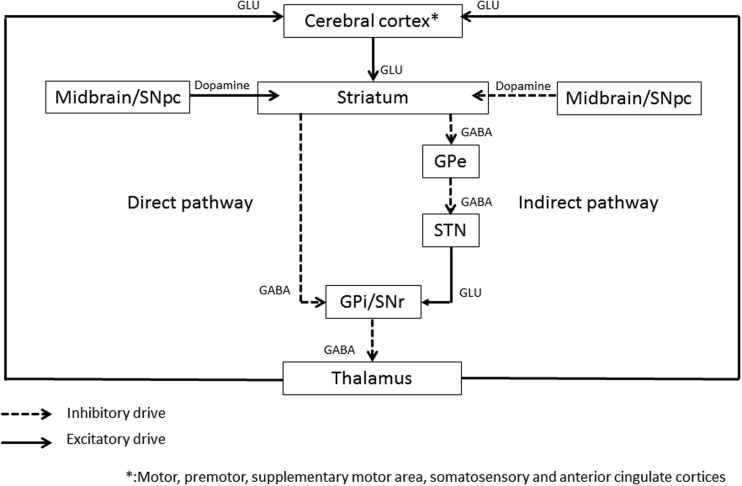
Dystonias represent a heterogeneous group of movement disorders responsible for sustained muscle contraction, abnormal postures, and muscle twists. It can affect focal or segmental body parts or be generalized. Primary dystonia is the most common form of dystonia but it can also be secondary to metabolic or structural dysfunction, the consequence of a drug's side-effect or of genetic origin. The pathophysiology is still not elucidated. Based on lesion studies, dystonia has been regarded as a pure motor dysfunction of the basal ganglia loop. However, basal ganglia lesions do not consistently produce dystonia and lesions outside basal ganglia can lead to dystonia; mild sensory abnormalities have been reported in the dystonic limb and imaging studies have shown involvement of multiple other brain regions including the cerebellum and the cerebral motor, premotor and sensorimotor cortices. Transcranial magnetic stimulation (TMS) is a non-invasive technique of brain stimulation with a magnetic field applied over the cortex allowing investigation of cortical excitability. Hyperexcitability of contralateral motor cortex has been suggested to be the trigger of focal dystonia. High or low frequency repetitive TMS (rTMS) can induce excitatory or inhibitory lasting effects beyond the time of stimulation and protocols have been developed having either a positive or a negative effect on cortical excitability and associated with prevention of cell death, γ-aminobutyric acid (GABA) interneurons mediated inhibition and brain-derived neurotrophic factor modulation. rTMS studies as a therapeutic strategy of dystonia have been conducted to modulate the cerebral areas involved in the disease. Especially, when applied on the contralateral (pre)-motor cortex or supplementary motor area of brains of small cohorts of dystonic patients, rTMS has shown a beneficial transient clinical effect in association with restrained motor cortex excitability. TMS is currently a valuable tool to improve our understanding of the pathophysiology of dystonia but large controlled studies using sham stimulation are still necessary to delineate the place of rTMS in the therapeutic strategy of dystonia. In this review, we will focus successively on the use of TMS as a tool to better understand pathophysiology, and the use of rTMS as a therapeutic strategy.
肌张力障碍是一组异质性的运动障碍,可导致肌肉持续收缩、异常姿势和肌肉扭曲。它可影响局部或节段性身体部位,也可为全身性的。原发性肌张力障碍是肌张力障碍最常见的形式,但也可能继发于代谢或结构功能障碍、药物副作用或遗传因素。其病理生理学仍未阐明。基于病变研究,肌张力障碍一直被视为基底神经节环路的单纯运动功能障碍。然而,基底神经节病变并不总是导致肌张力障碍,基底神经节以外的病变也可导致肌张力障碍;肌张力障碍肢体已报告有轻度感觉异常,影像学研究显示包括小脑、大脑运动皮质、运动前皮质和感觉运动皮质在内的多个其他脑区也有受累。经颅磁刺激(TMS)是一种非侵入性脑刺激技术,通过在皮质上方施加磁场来研究皮质兴奋性。对侧运动皮质的兴奋性过高被认为是局灶性肌张力障碍的触发因素。高频或低频重复经颅磁刺激(rTMS)可在刺激时间之外诱导兴奋性或抑制性持久效应,并且已经开发出了对皮质兴奋性有正向或负向影响并与预防细胞死亡、γ-氨基丁酸(GABA)中间神经元介导的抑制和脑源性神经营养因子调节相关的方案。作为肌张力障碍治疗策略的rTMS研究已用于调节与该疾病相关的脑区。特别是,当应用于一小群肌张力障碍患者大脑的对侧(前)运动皮质或辅助运动区时,rTMS已显示出有益的短暂临床效果,并伴有运动皮质兴奋性的抑制。目前,TMS是增进我们对肌张力障碍病理生理学理解的有价值工具,但仍需要使用假刺激的大型对照研究来确定rTMS在肌张力障碍治疗策略中的地位。在本综述中,我们将依次重点介绍TMS作为更好地理解病理生理学的工具的应用,以及rTMS作为治疗策略的应用。