Janoudi Ghayath, Amegatse William, McIntosh Brendan, Sehgal Chander, Richter Trevor
CADTH, 865 Carling Ave., Suite 600, Ottawa, ON, K1S 5S8, Canada.
Orphanet J Rare Dis. 2016 Dec 1;11(1):164. doi: 10.1186/s13023-016-0539-3.
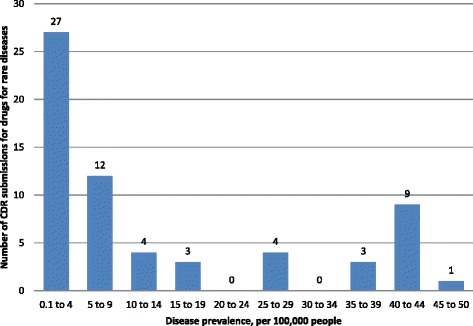
A shift in biochemical research towards drugs for rare diseases has created new challenges for the pharmaceutical industry, government regulators, health technology assessment agencies, and public and private payers. In this article, we aim to comprehensively review, characterize, identify possible trends, and explore reasons for negative reimbursement recommendations in submissions made to the Common Drug Review (CDR) for drugs for rare diseases (DRD) at the Canadian Agency for Drugs and Technologies in Health (CADTH), a publicly funded pan-Canadian health technology assessment agency. A public database (cadth.ca) was screened to identify DRD submissions to CDR. A diseases prevalence of ≤50 per 100,000 people was considered a rare disease. We calculated descriptive statistics for prevalence, study design, study size, treatment cost, reimbursement recommendation types, and reasons for negative reimbursement recommendations.
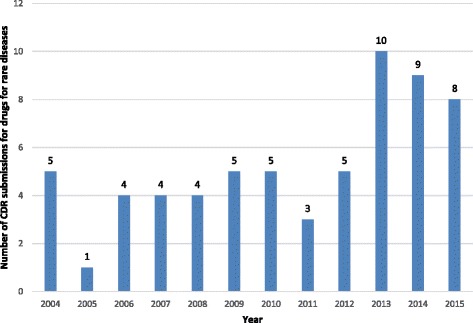
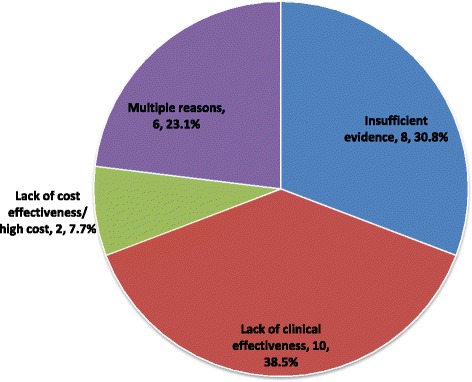
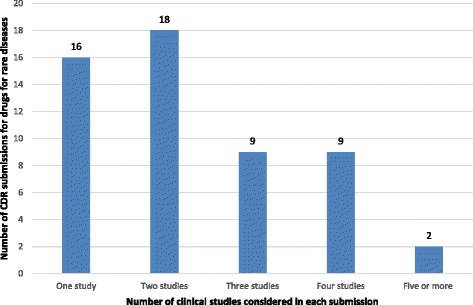
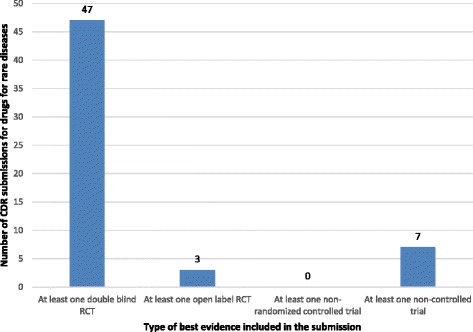
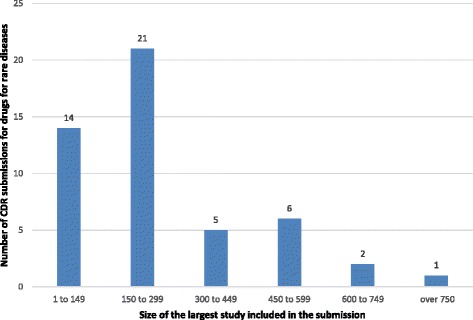
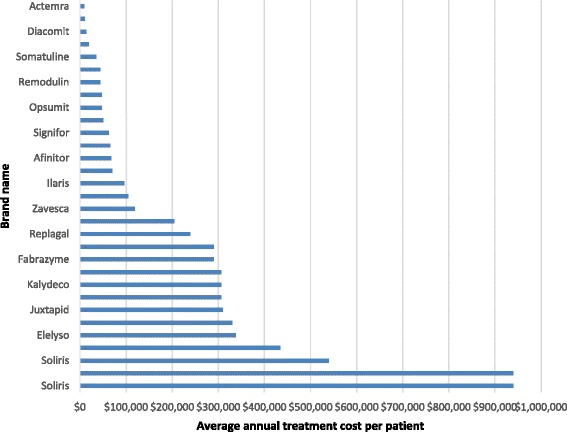
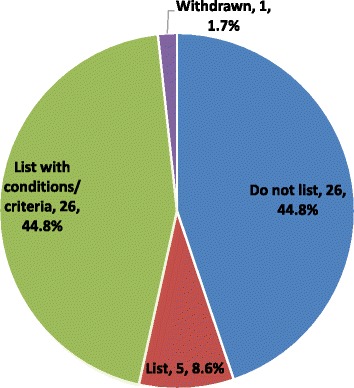
From 2004 to 2015, 63 of 434 submissions to the CDR were for DRD (range: 1 submission in 2005 to 10 submissions in 2013). Most (74.6%) submissions included at least one double-blind randomized controlled trial (RCT). The average study size was 190 patients (range: 20 to 742). The average annual treatment cost was C$215,631 (range: $9,706 to $940,084). Reimbursement recommendations were positive for 54% of the submissions. Negative reimbursement recommendations were made due to a lack of clinical effectiveness (38.5%), insufficient evidence (30.8%), multiple reasons (23.1%), or lack of cost effectiveness/high cost (7.7%).
The number of DRD submissions to CDR increased since 2013; from 4 to 5 per year between 2004 and 2012, to 10, 9, and 8 in 2013, 2014, and 2015 respectively. More than half of DRD submissions received positive reimbursement recommendation. Poor quality evidence and/or lack of supportive clinical evidence was at least partly responsible for a negative reimbursement recommendation in all cases. Although the average cost of DRD treatments was high, high cost was a reason for a negative reimbursement recommendation in only two (7.7%) of negative reimbursement recommendations.
生物化学研究向罕见病药物的转变给制药行业、政府监管机构、卫生技术评估机构以及公共和私人支付方带来了新的挑战。在本文中,我们旨在全面回顾、描述、识别可能的趋势,并探究向加拿大卫生技术评估署(CADTH)的常见药物审查(CDR)提交的罕见病药物(DRD)申请中报销建议为负面的原因。CADTH是一家由公共资金资助的泛加拿大卫生技术评估机构。我们筛选了一个公共数据库(cadth.ca)以识别提交给CDR的DRD申请。每10万人中患病率≤50的疾病被视为罕见病。我们计算了患病率、研究设计、研究规模、治疗成本、报销建议类型以及负面报销建议原因的描述性统计数据。
2004年至2015年期间,提交给CDR的434份申请中有63份是关于DRD的(范围:2005年1份申请至2013年10份申请)。大多数(74.6%)申请至少包含一项双盲随机对照试验(RCT)。平均研究规模为190名患者(范围:20至742)。平均每年治疗成本为215,6