Kazianka L, Drucker C, Skrabs C, Thomas W, Melchardt T, Struve S, Bergmann M, Staber P B, Porpaczy E, Einberger C, Heinz M, Hauswirth A, Raderer M, Pabinger I, Thalhammer R, Egle A, Wendtner C-M, Follows G, Hoermann G, Quehenberger P, Jilma B, Jaeger U
Department of Medicine I, Division of Hematology and Hemostaseology, Medical University of Vienna, Vienna, Austria.
Comprehensive Cancer Center, Medical University of Vienna, Vienna, Austria.
Leukemia. 2017 May;31(5):1117-1122. doi: 10.1038/leu.2016.316. Epub 2016 Nov 2.
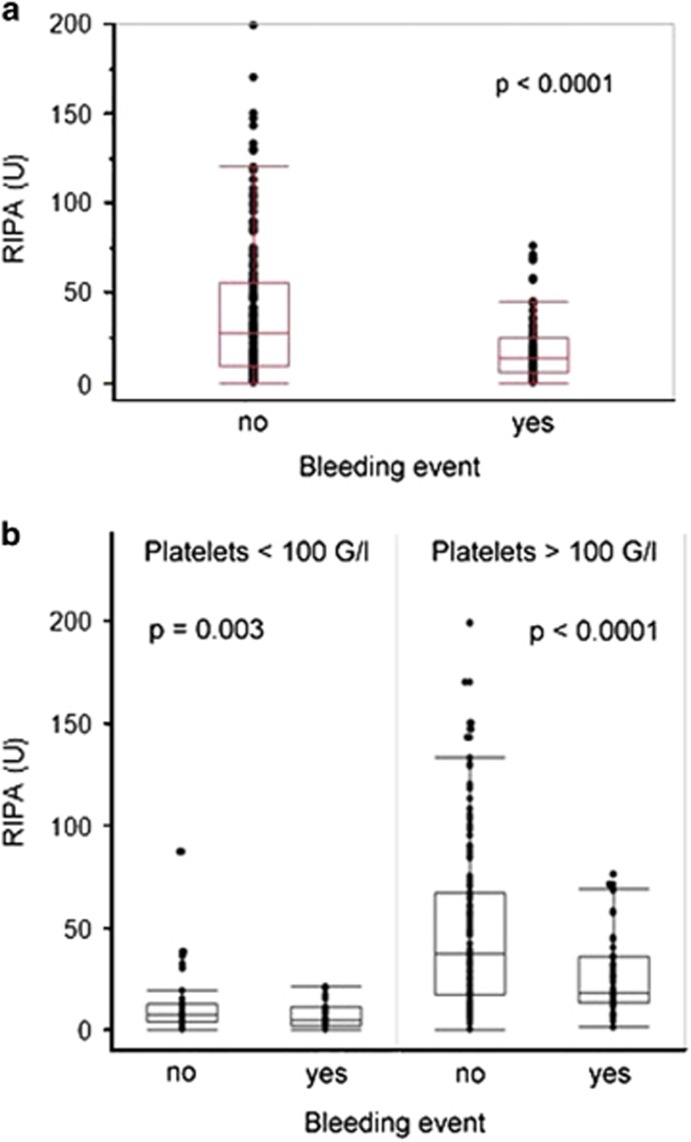
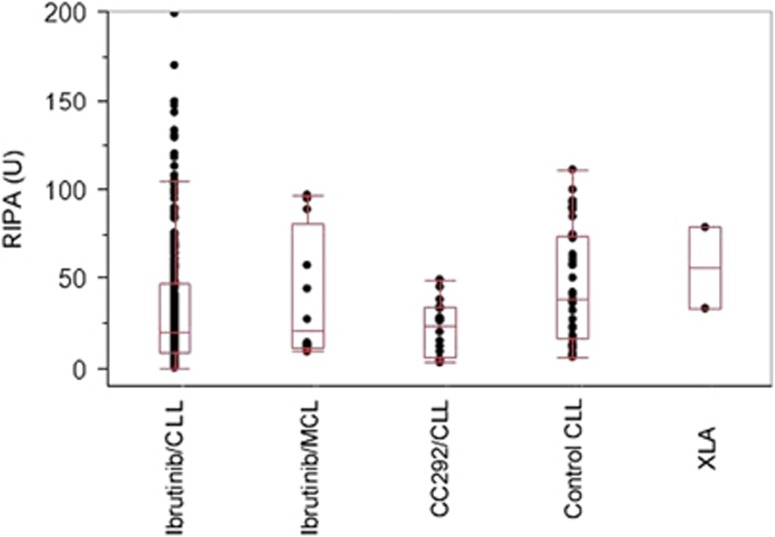
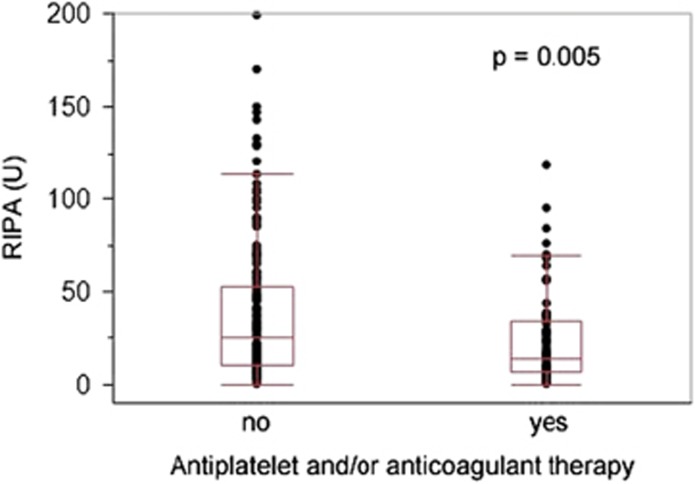
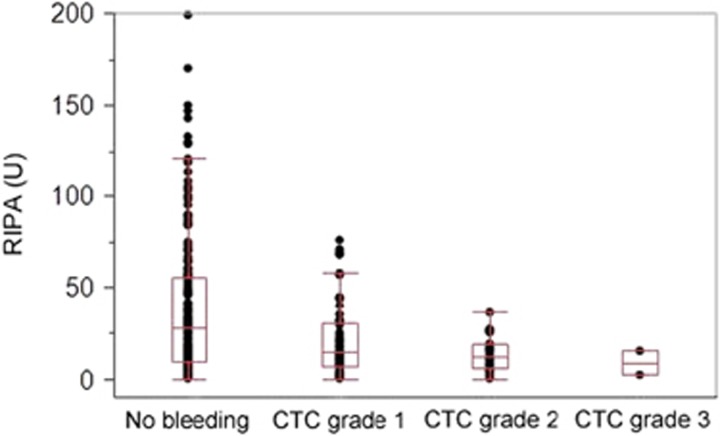
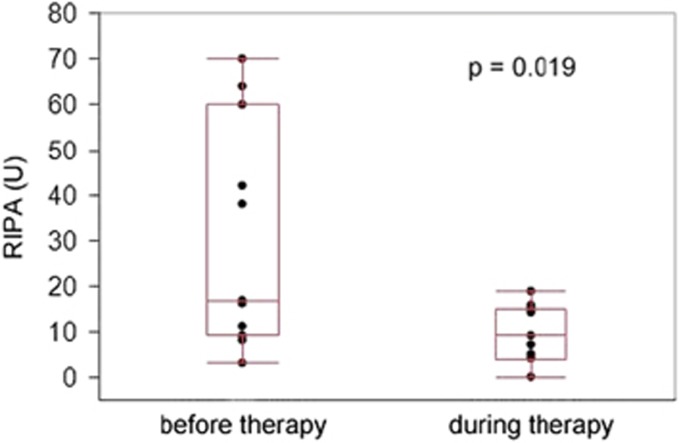
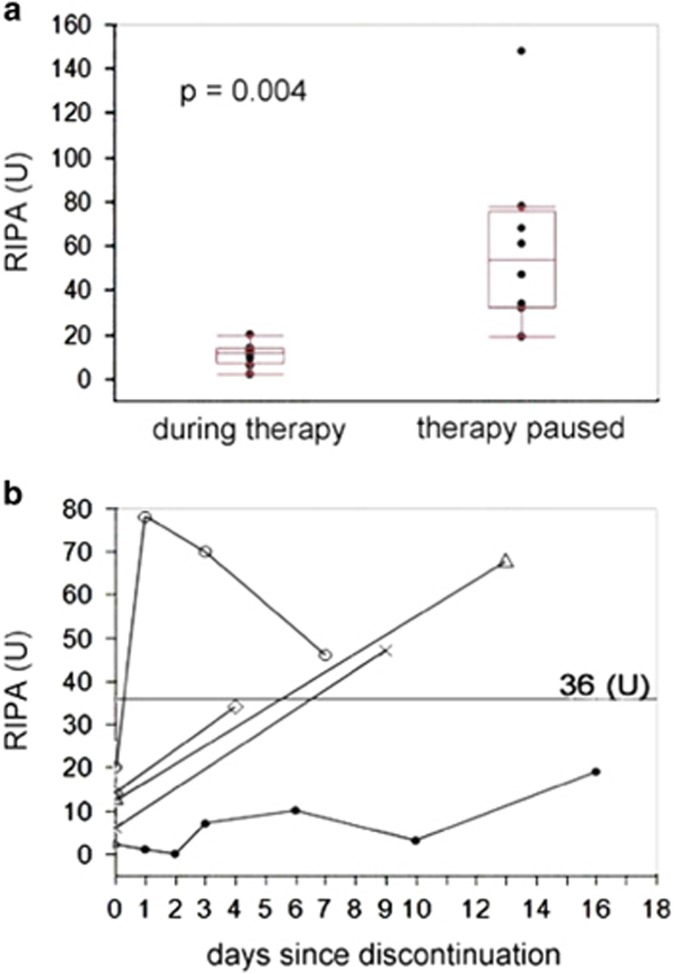
Bleeding because of impaired platelet function is a major side effect of the Bruton's tyrosine kinase (BTK) inhibitor ibrutinib. We quantitatively assessed ristocetin-induced platelet aggregation (RIPA) in 64 patients with chronic lymphocytic leukemia (CLL) under ibrutinib at 287 time points. Eighty-seven bleeding episodes in 39 patients were registered (85 Common Toxicity Criteria (CTC) grade 1 or 2, 2 CTC grade 3) during a median observation period of 10.9 months. At times of bleeding, RIPA values were significantly lower (14 vs 28 U; P<0.0001). RIPA was impaired in patients receiving concomitant antiplatelet therapy or anticoagulation (14 vs 25 U, P=0.005). A gradual decline of median RIPA values was observed with increasing bleeding severity. Importantly, no CTC grade 2 or 3 bleeding were observed with RIPA values of >36 U. Sequential monitoring indicated a decrease of RIPA values from a median of 17 to 9 U within 2 weeks after initiation of treatment as well as an increase above the critical threshold of 36 U within 7 days when ibrutinib was paused. Low RIPA values were similar during treatment with another BTK inhibitor, CC292. Quantitative assessment of platelet function is a practical tool to monitor bleeding tendency under BTK-inhibitor therapy.
由于血小板功能受损导致的出血是布鲁顿酪氨酸激酶(BTK)抑制剂依鲁替尼的主要副作用。我们在287个时间点对64例接受依鲁替尼治疗的慢性淋巴细胞白血病(CLL)患者进行了瑞斯托霉素诱导的血小板聚集(RIPA)定量评估。在中位观察期10.9个月内,39例患者共发生87次出血事件(85例为常见毒性标准(CTC)1级或2级,2例为CTC 3级)。出血时,RIPA值显著降低(14 vs 28 U;P<0.0001)。接受联合抗血小板治疗或抗凝治疗的患者RIPA受损(14 vs 25 U,P=0.005)。随着出血严重程度增加,观察到RIPA中位数逐渐下降。重要的是,RIPA值>36 U时未观察到CTC 2级或3级出血。连续监测表明,治疗开始后2周内RIPA值从中位数17 U降至9 U,依鲁替尼暂停使用7天内RIPA值升至关键阈值36 U以上。使用另一种BTK抑制剂CC292治疗期间,低RIPA值相似。血小板功能的定量评估是监测BTK抑制剂治疗下出血倾向的实用工具。