Ali Abdelhamid Yasmine, Phillips Liza, Horowitz Michael, Deane Adam
Intensive Care Unit, Royal Adelaide Hospital, North Terrace, Adelaide, South Australia 5000 Australia ; Discipline of Acute Care Medicine, The University of Adelaide, North Terrace, Adelaide, South Australia 5000 Australia.
Endocrine and Metabolic Unit, Royal Adelaide Hospital, North Terrace, Adelaide, South Australia 5000 Australia ; Discipline of Medicine, The University of Adelaide, North Terrace, Adelaide, South Australia 5000 Australia.
Pilot Feasibility Stud. 2016 Oct 13;2:62. doi: 10.1186/s40814-016-0104-9. eCollection 2016.
Many patients who survive the intensive care unit (ICU) experience long-term complications such as peripheral neuropathy and nephropathy which represent a major source of morbidity and affect quality of life adversely. Similar pathophysiological processes occur frequently in ambulant patients with diabetes mellitus who have never been critically ill. Some 25 % of all adult ICU patients have diabetes, and it is plausible that ICU survivors with co-existing diabetes are at heightened risk of sequelae from their critical illness. ICU follow-up clinics are being progressively implemented based on the concept that interventions provided in these clinics will alleviate the burdens of survivorship. However, there is only limited information about their outcomes. The few existing studies have utilised the expertise of healthcare professionals primarily trained in intensive care and evaluated heterogenous cohorts. A shared care model with an intensivist- and diabetologist-led clinic for ICU survivors with type 2 diabetes represents a novel targeted approach that has not been evaluated previously. Prior to undertaking any definitive study, it is essential to establish the feasibility of this intervention.
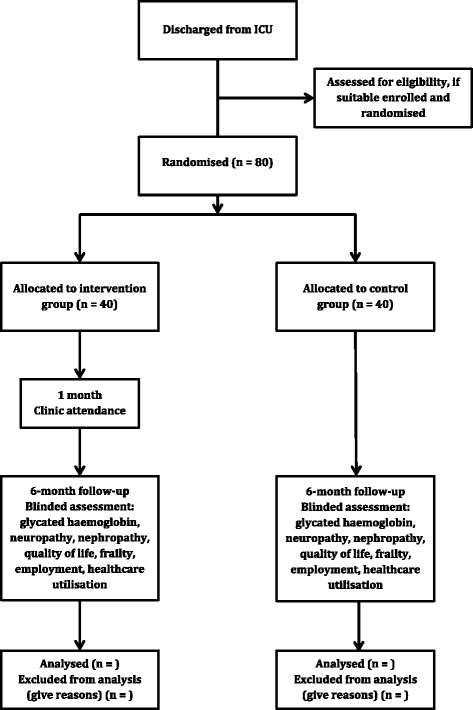
This will be a prospective, randomised, parallel, open-label feasibility study. Eligible patients will be approached before ICU discharge and randomised to the intervention (attending a shared care follow-up clinic 1 month after hospital discharge) or standard care. At each clinic visit, patients will be assessed independently by both an intensivist and a diabetologist who will provide screening and targeted interventions. Six months after discharge, all patients will be assessed by blinded assessors for glycated haemoglobin, peripheral neuropathy, cardiovascular autonomic neuropathy, nephropathy, quality of life, frailty, employment and healthcare utilisation. The primary outcome of this study will be the recruitment and retention at 6 months of all eligible patients.
This study will provide preliminary data about the potential effects of critical illness on chronic glucose metabolism, the prevalence of microvascular complications, and the impact on healthcare utilisation and quality of life in intensive care survivors with type 2 diabetes. If feasibility is established and point estimates are indicative of benefit, funding will be sought for a larger, multi-centre study.
ANZCTR ACTRN12616000206426.
许多在重症监护病房(ICU)存活下来的患者会经历长期并发症,如周围神经病变和肾病,这些并发症是发病的主要原因,并对生活质量产生不利影响。类似的病理生理过程在从未患过重症的糖尿病门诊患者中也经常出现。所有成年ICU患者中约25%患有糖尿病,因此,患有糖尿病的ICU幸存者因重症而出现后遗症的风险可能更高。基于这些诊所提供的干预措施将减轻幸存者负担的理念,ICU随访诊所正在逐步实施。然而,关于其效果的信息有限。现有的少数研究主要利用了在重症监护方面接受过培训的医疗专业人员的专业知识,并评估了异质性队列。由重症监护专家和糖尿病专家主导的2型糖尿病ICU幸存者共享护理模式是一种新的靶向方法,此前尚未进行过评估。在进行任何确定性研究之前,确定这种干预措施的可行性至关重要。
这将是一项前瞻性、随机、平行、开放标签的可行性研究。符合条件的患者将在ICU出院前被纳入研究,并随机分为干预组(出院后1个月参加共享护理随访诊所)或标准护理组。在每次诊所就诊时,患者将由重症监护专家和糖尿病专家独立评估,他们将提供筛查和针对性干预措施。出院6个月后,所有患者将由盲法评估人员评估糖化血红蛋白、周围神经病变、心血管自主神经病变、肾病、生活质量、虚弱程度、就业情况和医疗保健利用情况。本研究的主要结果将是所有符合条件的患者在6个月时的招募和留存情况。
本研究将提供关于重症对慢性葡萄糖代谢的潜在影响、微血管并发症的患病率以及对2型糖尿病ICU幸存者的医疗保健利用和生活质量影响的初步数据。如果确定了可行性且点估计表明有获益,将寻求资金进行更大规模的多中心研究。
澳大利亚和新西兰临床试验注册中心(ANZCTR)注册号:ACTRN12616000206426。