Cooles Faye A H, Anderson Amy E, Drayton Tracey, Harry Rachel A, Diboll Julie, Munro Lee, Thalayasingham Nishanthi, Östör Andrew J K, Isaacs John D
Institute of Cellular Medicine, Newcastle University and National Institute for Health Research Newcastle Biomedical Research Centre at Newcastle upon Tyne Hospitals NHS Foundation Trust and Newcastle University, Newcastle upon Tyne, UK.
Addenbrooke's NHS trust, Cambridge, UK.
Arthritis Res Ther. 2016 Dec 20;18(1):302. doi: 10.1186/s13075-016-1188-6.
Alemtuzumab, an anti-CD52 monoclonal antibody, was administered to patients with RA between 1991 and 1994. We have followed a cohort of recipients since that time and previously reported significant delays in immune reconstitution. Here we report >20 years of follow-up data from this unique cohort.
Surviving alemtuzumab recipients were age, sex and disease duration matched with RA controls. Updated mortality and morbidity data were collected for alemtuzumab recipients. For both groups antigenic responses were assessed following influenza, Pneumovax II and combined diphtheria/tetanus/poliovirus vaccines. Circulating cytokines and lymphocyte subsets were also quantified.
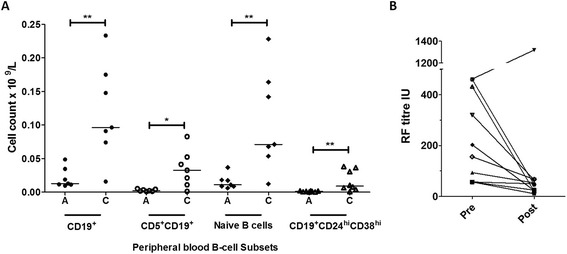
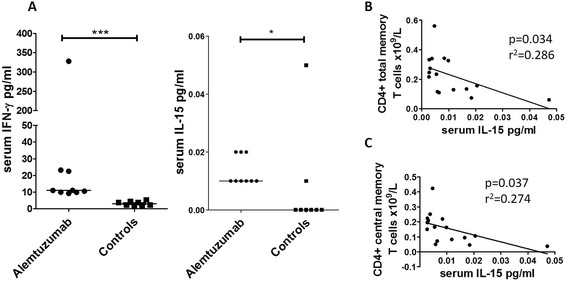
Of 16 surviving alemtuzumab recipients, 13 were recruited: 9 recipients underwent a full clinical assessment and 4 had case notes review only. Since our last review 10 patients had died from causes of death consistent with long-standing RA, and no suggestion of compromised immune function. Compared with controls the alemtuzumab cohort had significantly reduced CD4 and CD8 central memory T-cells, CD5 B cells, naïve B cells and CD19CD24CD38 transitional (putative regulatory) B cells. Nonetheless vaccine responses were comparable between groups. There were significantly higher serum IL-15 and IFN-γ levels in the alemtuzumab cohort. IL-15 levels were inversely associated with CD4 total memory and central memory T cells.
After 20 years the immune system of alemtuzumab recipients continues to show differences from disease controls. Nonetheless mortality and morbidity data, alongside vaccination responses, do not suggest clinical immune compromise. As lymphodepleting therapies, including alemtuzumab, continue to be administered this work is important with regard to long-term immune monitoring and stages of immune recovery.
1991年至1994年间,抗CD52单克隆抗体阿仑单抗被用于治疗类风湿关节炎(RA)患者。自那时起,我们对一组接受该治疗的患者进行了随访,此前报告了免疫重建存在显著延迟。在此,我们报告该独特队列超过20年的随访数据。
存活的阿仑单抗接受者在年龄、性别和病程上与RA对照组相匹配。收集阿仑单抗接受者最新的死亡率和发病率数据。对两组患者在接种流感疫苗、肺炎球菌疫苗II以及白喉/破伤风/脊髓灰质炎联合疫苗后评估抗原反应。还对循环细胞因子和淋巴细胞亚群进行了定量分析。
在16名存活的阿仑单抗接受者中,招募了13名:9名接受者接受了全面的临床评估,4名仅进行了病例记录复查。自我们上次复查以来,10名患者死于与长期RA相符的死因,且未提示免疫功能受损。与对照组相比,阿仑单抗队列的CD4和CD8中央记忆T细胞、CD5 B细胞、幼稚B细胞以及CD19CD24CD38过渡性(假定调节性)B细胞显著减少。尽管如此,两组之间的疫苗反应相当。阿仑单抗队列的血清IL-15和IFN-γ水平显著更高。IL-15水平与CD4总记忆和中央记忆T细胞呈负相关。
20年后,阿仑单抗接受者的免疫系统与疾病对照组相比仍存在差异。尽管如此,死亡率和发病率数据以及疫苗反应均未提示临床免疫受损。随着包括阿仑单抗在内的淋巴细胞清除疗法持续应用,这项工作对于长期免疫监测和免疫恢复阶段具有重要意义。