Masel Eva Katharina, Huber Patrick, Engler Tobias, Watzke Herbert Hans
Clinical Division of Palliative Care, Department of Internal Medicine I, Medical University of Vienna, Vienna, Austria.
J Pain Res. 2016 Dec 12;9:1215-1220. doi: 10.2147/JPR.S120343. eCollection 2016.
Decisions on the intensity of analgesic therapy and judgments regarding its efficacy are difficult at the end of life, when many patients are not fully conscious and pain is a very common symptom. In healthy individuals and in postoperative settings, nociception and subsequent pain relief have been shown to induce changes in the autonomic nervous system (ANS), which can be detected by measuring heart rate variability (HRV).
The changes in the ANS were studied by measuring HRV during opioid therapy for cancer breakthrough pain (CBTP) in palliative-care patients with cancer and compared these changes with patient-reported pain levels on a numeric rating scale (NRS).
The study included ten patients with advanced cancer and baseline opioid therapy. In each patient, a 24-hour peak-to-peak HRV measurement with a sampling rate of 4,000 Hz was performed. High frequency (HF), low frequency (LF), total power, pNN50 (indicating parasympathetic activity), and log LF/HF were obtained in two intervals prior to therapy and in four intervals thereafter. Intensity of CBTP was recorded using a patient-reported NRS prior to therapy and 30 minutes afterward.
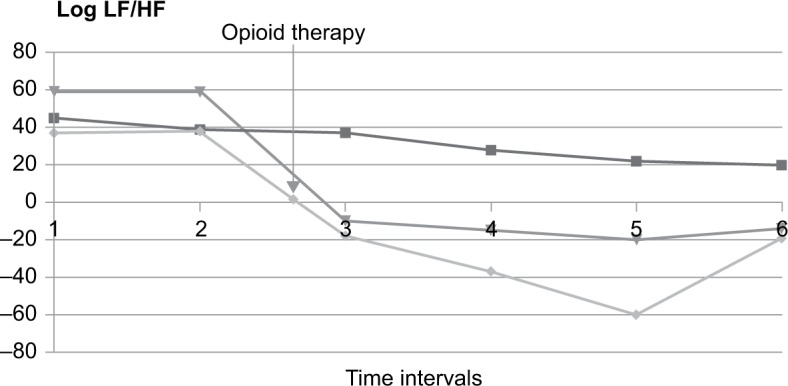
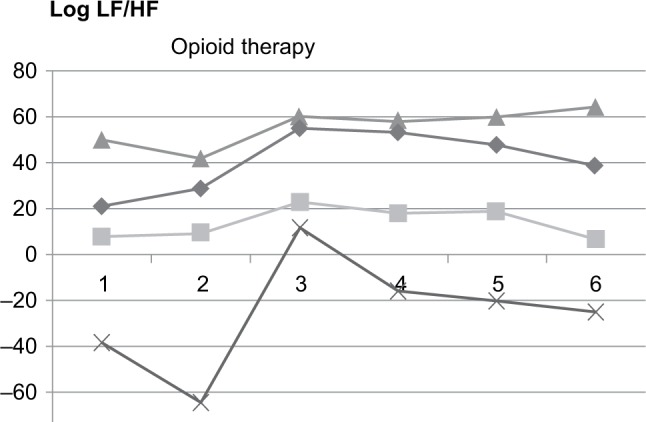
CBTP occurred in seven patients (three males and four females; mean age: 62 ± 5.2 years) and was treated with opioids. A highly significant positive correlation was found between opioid-induced reduction in patient-reported pain intensity based on NRS and changes in log LF/HF ( > 0.700; < 0.05). Log LF/HF decreased in patients who had a reduction in pain of >2 points on the NRS but remained unchanged in the other patients.
Our data suggest that log LF/HF may be a useful surrogate marker for alleviation of CBTP in patients with advanced cancer and might allow detection of pain without active contribution from patients.
在生命末期,当许多患者意识不完全清醒且疼痛是非常常见的症状时,关于镇痛治疗强度的决策及其疗效判断都很困难。在健康个体和术后环境中,伤害感受及随后的疼痛缓解已被证明会引起自主神经系统(ANS)的变化,这可以通过测量心率变异性(HRV)来检测。
通过测量癌症姑息治疗患者癌痛爆发性疼痛(CBTP)的阿片类药物治疗期间的HRV来研究ANS的变化,并将这些变化与患者在数字评分量表(NRS)上报告的疼痛水平进行比较。
该研究纳入了10例接受阿片类药物基础治疗的晚期癌症患者。对每位患者进行了采样率为4000Hz的24小时峰峰值HRV测量。在治疗前的两个时间段以及治疗后的四个时间段获取高频(HF)、低频(LF)、总功率、pNN50(指示副交感神经活动)和对数LF/HF。在治疗前和治疗后30分钟使用患者报告的NRS记录CBTP的强度。
7例患者(3例男性和4例女性;平均年龄:62±5.2岁)发生CBTP并接受了阿片类药物治疗。基于NRS的阿片类药物引起的患者报告疼痛强度降低与对数LF/HF的变化之间存在高度显著的正相关(>0.700;<0.05)。NRS疼痛评分降低超过2分的患者对数LF/HF降低,而其他患者则保持不变。
我们的数据表明,对数LF/HF可能是晚期癌症患者CBTP缓解的有用替代指标,并且可能允许在患者没有主动参与的情况下检测疼痛。