Lischalk Jonathan W, Woo Stephanie M, Kataria Shaan, Aghdam Nima, Paydar Ima, Repka Michael C, Anderson Eric D, Collins Brian T
Department of Radiation Medicine, Georgetown University Hospital, Lower Level Bles, 3800 Reservoir Road, N.W, Washington, DC 20007 USA.
Division of Pulmonary, Critical Care, and Sleep Medicine, Georgetown University Hospital, Pasquerilla Healthcare Center, 5th floor, 3800 Reservoir Road, N.W., Washington, DC 20007 USA.
J Radiat Oncol. 2016;5(4):379-387. doi: 10.1007/s13566-016-0273-4. Epub 2016 Aug 20.
Stereotactic body radiation therapy (SBRT) for stage I non-small cell lung cancer (NSCLC) is considered standard of care in the medically inoperable patient population. Multiple methods of SBRT delivery exist including fiducial-based tumor tracking, which allows for smaller treatment margins and avoidance of patient immobilization devices. We explore the long-term clinical outcomes of this novel fiducial-based SBRT method.
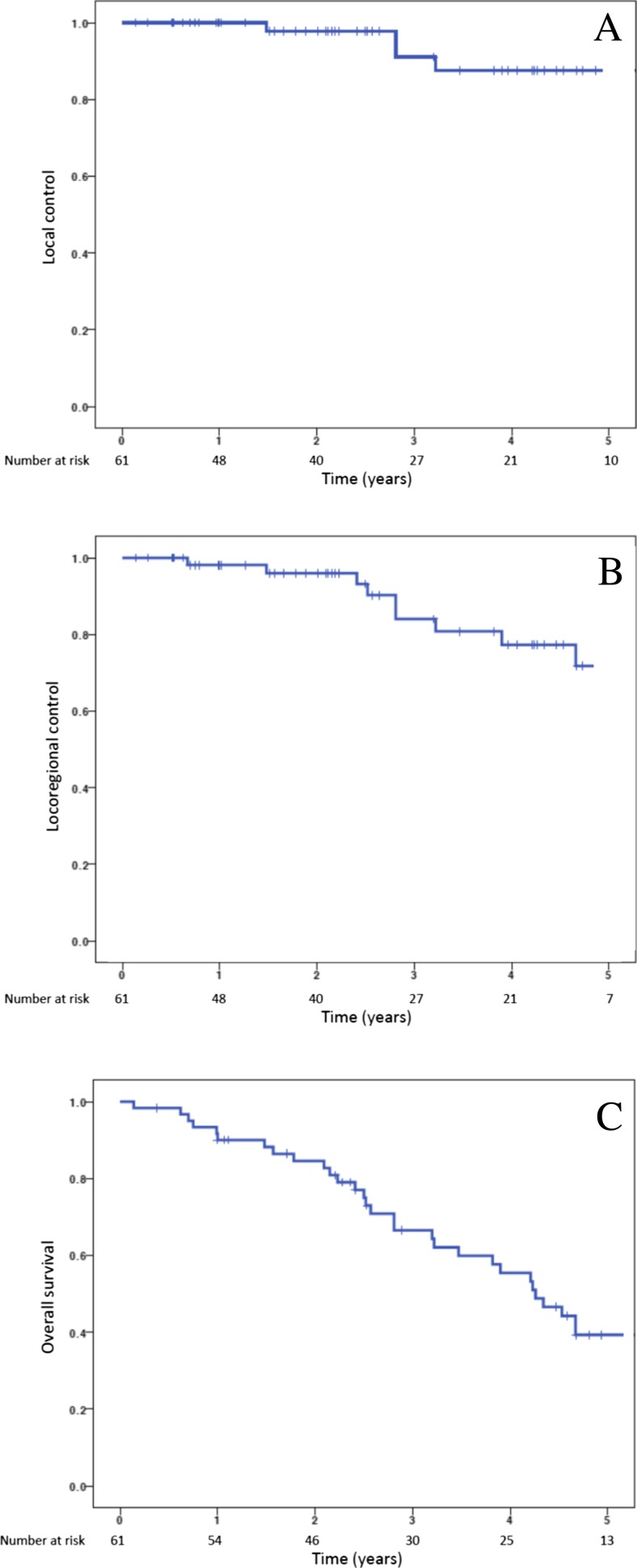
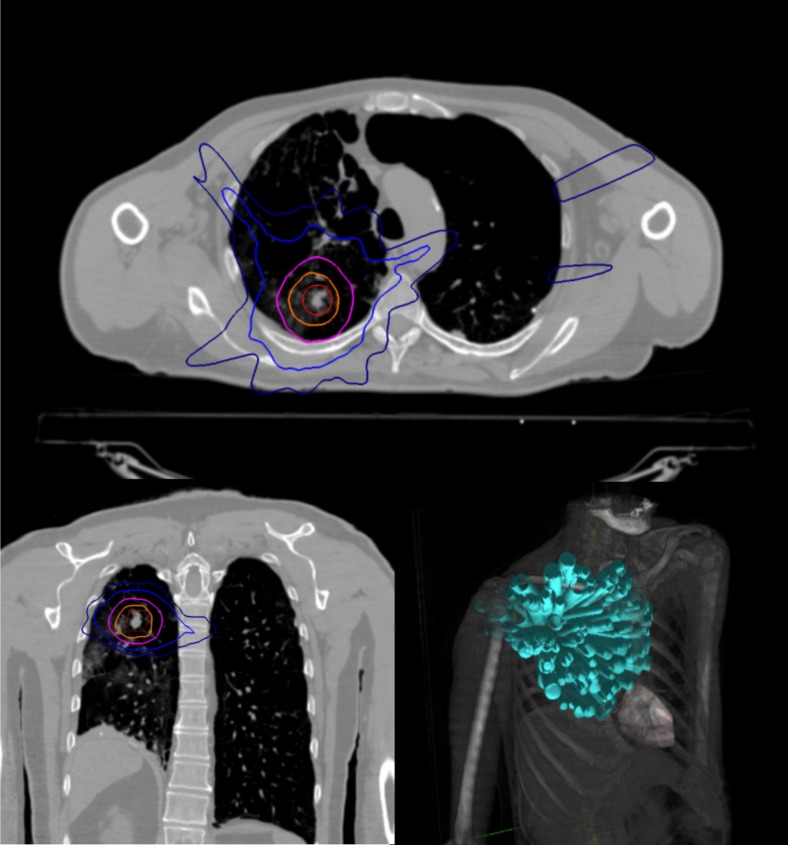
In this single institutional retrospective review, we detail the outcomes of medically inoperable pathologically confirmed stage I NSCLC. Patients were treated with the Cyberknife SBRT system using a planning target volume (PTV) defined as a 5-mm expansion from gross tumor volume (GTV) without creation of an internal target volume (ITV). Dose was delivered in three or five equal fractions of 10 to 20 Gy. Pretreatment and posttreatment pulmonary function test (PFT) changes and evidence of late radiological rib fractures were analyzed for the majority of patients. Actuarial local control, locoregional control, distant control, and overall survival were calculated using the Kaplan-Meier method.
Sixty-one patients with a median age of 75 years were available for analysis. The majority (80 %) of patients were deemed to be medically inoperable due to underlying pulmonary dysfunction. Eleven patients (18 %) developed symptomatic pneumothoraces secondary to fiducial placement under CT guidance, which precipitously dropped to 0 % following transition to bronchoscopic fiducial placement. The 2-year rib fracture risk was 21.4 % with a median time to rib fracture of 2.9 years. PFTs averaged over all patients and parameters demonstrated small absolute declines, 5.7 % averaged PFT decline, at approximately 1 year of follow-up, but only the diffusing capacity of lung for carbon monoxide (DL) demonstrated a statistically significant decline (10.29 vs. 9.01 mL/min/mmHg, = 0.01). Five-year local control, locoregional control, and overall survival were 87.6, 71.8, and 39.3 %, respectively.
Despite reduced treatment margins and lack of patient immobilization, SBRT with fiducial-based tumor tracking achieves clinically comparable long-term outcomes to other linac-based SBRT approaches.
立体定向体部放射治疗(SBRT)用于治疗 I 期非小细胞肺癌(NSCLC),在医学上无法手术的患者群体中被视为标准治疗方法。SBRT 有多种实施方式,包括基于基准标记的肿瘤追踪,这种方法可缩小治疗边界并避免使用患者固定装置。我们探讨了这种基于新型基准标记的 SBRT 方法的长期临床疗效。
在这项单机构回顾性研究中,我们详细阐述了医学上无法手术的经病理证实的 I 期 NSCLC 患者的治疗结果。患者使用射波刀 SBRT 系统进行治疗,计划靶区(PTV)定义为在大体肿瘤体积(GTV)基础上外放 5 毫米,不创建内部靶区(ITV)。剂量分 3 或 5 等份给予,每次 10 至 20 戈瑞。对大多数患者分析了治疗前和治疗后肺功能测试(PFT)的变化以及晚期放射性肋骨骨折的证据。使用 Kaplan-Meier 方法计算精算局部控制率、区域控制率、远处控制率和总生存率。
61 例患者可供分析,中位年龄 75 岁。大多数患者(80%)因潜在的肺功能障碍被认为无法进行手术。11 例患者(18%)在 CT 引导下放置基准标记后出现症状性气胸,在改用支气管镜下放置基准标记后,这一比例急剧降至 0%。2 年肋骨骨折风险为 21.4%,肋骨骨折的中位时间为 2.9 年。所有患者和各项参数的平均 PFT 在随访约 1 年时平均绝对下降 5.7%,但只有肺一氧化碳弥散量(DL)有统计学显著下降(10.29 对比 9.01 毫升/分钟/毫米汞柱,P = 0.01)。5 年局部控制率、区域控制率和总生存率分别为 87.6%、71.8%和 39.3%。
尽管治疗边界缩小且未使用患者固定装置,但基于基准标记肿瘤追踪的 SBRT 与其他基于直线加速器的 SBRT 方法相比,在临床上可取得相当的长期疗效。